Red Yeast Rice is a preparation made from a yeast that is commercially grown on rice grains. The rice and yeast, which is deep red in color, are ground up into a red powder. Red yeast rice has been found to support naturally support healthy blood lipid levels already in the normal range.*
Fueled by extensive studies, scientific evidence demonstrating the safety, tolerability, and efficacy of red yeast rice (RYR) continues to mount.2-6,12 The first use of RYR was documented in 800 A.D., during the Tang Dynasty. Subsequently, during the Ming Dynasty (1368- 1644), the manufacturing process was published in the ancient Chinese pharmacopoeia. The typical Asian diet contains 14-55 grams of naturally occurring Red Yeast Rice per day.7
The potential benefits of consuming Red Yeast Rice or its supplement form, RYRE (red yeast rice extract), are multi-faceted. In traditional Chinese medicine, the powdered form is called Hong Qu, Hong Mi, or Chi Qu. Considered sweet, acidic, and warm, it is used to strengthen the spleen and stomach, thereby promoting digestion, invigorating blood circulation, and eliminating blood stasis.8 In western medicine, Red Yeast Rice has been shown to downregulate adipogenic transcription factors such as PPAR gamma and other genes that differentiate adipocytes.9
Researchers believe the most active constituents of RYR are its various monacolins, particularly monacolin K, which the body converts to ß-hydroxy acid. A study utilizing hamsters concluded that “the activity of RYR is, at least, partially mediated by enhancement of acidic sterol excretion.”10 RYR also contains various pigments, tannins, phytochemicals such as sterols and isoflavones, and mono-unsaturated fatty acids, all of which may work synergistically with the monacolins.4,8
Since 1996, there have been no fewer than nine randomized, controlled RYR/RYRE trials involving thousands of subjects. Studies since the 1970s have demonstrated that RYRE supports healthy blood lipid levels already in the normal range. The medical literature associated with these studies includes comparative, case series, and dosing studies.2-12
In its natural state, RYRE may contain the mycotoxin, citrinin, a secondary metabolite of the Monascusspecies.3 Accordingly, any manufacturer of Red Yeast Rice should carefully test and document each and every batch of RYRE raw material to comply with strict limits for citrinin and to assure its safety. If you are taking a Red Yeast Rice supplement, or looking for one, be sure to only select one that is labeled “citrinin-free.”
Dose: It is often recommended to take anywhere between 800 and 4,000mg of Red Yeast Rice.
References
Becker DJ, et.al. Red yeast rice for dyslipidemia in statin-intolerant patients: a randomized trial. Ann Intern Med. 2009 Jun 16;150(12):830-9, W147-9. [PMID: 19528562]
Bianchi A. Extracts of Monascusus purpureus beyond statins–profile of efficacy and safety of the use of extracts of Monascus purpureus. Chin J Integr Med. 2005 Dec;11(4):309-13. Review. [PMID: 16417786 ]
Wang TH, Lin TF. Monascus rice products. Adv Food Nutr Res. 2007;53:123- 59. Review. [PMID: 17900498]
Heber D, et al. Cholesterol-lowering effects of a proprietary Chinese red yeast rice dietary supplement. Am J Clin Nutr 1999;69:231-236. [PMID: 9989685]
A Monascus Purpureus rice preparation reduces serum cholesterol and triacylglycerols in elderly with primary hyperlipidemia: A randomized double- blind clinical trial. National Medical Association Scientific Assembly. August 1-6, 1998
Hung Qu (Monascus). Chen JK, Chen TT. Chinese Medical Herbology and Pharmacology. Art of Medicine Press. CA 2001:527-528
Jeon T, et al. Red yeast rice extracts suppress adipogenesis by down-regulating adipogenic transcription factors and gene expression in 3T3-L1 cells. Life Sci. 2004 Nov 12;75(26):3195-203 [PMID: 15488898]
Ma KY, et al. Red yeast rice increases excretion of bile acids in hamsters.
Biomed Environ Sci. 2009 Aug;22(4):269-77. [PMID: 19950521]
Halbert SC, et al. Tolerability of red yeast rice (2,400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previous statin intolerance. Am J Cardiol. 2010 Jan 15;105(2):198-204. Epub 2009 Nov 26. [PMID: 20102918]
Li JJ, et al. Chinese Coronary Secondary Prevention Study Group Beneficial impact of Xuezhikang on cardiovascular events and mortality in elderly hypertensive patients with previous myocardial infarction from the China Coronary Secondary Prevention Study (CCSPS). J. Clin Pharmacol. 2009 Aug;49(8):947-56. [PMID 19602720]
Vercelli L, et al. Chinese red rice depletes muscle coenzyme Q10 and maintains muscle damage after discontinuation of statin treatment. J Am Geriatr Soc.2006 Apr;54(4):718-20 [PMID: 16686894]”
Resveratrol turns off NADPH Oxidase which is one mechanism through which superoxide anion is made.
Resveratrol (3,5,4′-trihydroxystilbene) is a stilbenol derived from stilbene, a natural plant product. Resveratrol is found in varying amounts in grapes, various berries, plums, peanuts (and pines). Oral resveratrol is rapidly metabolized via sulfate conjugation by the intestine/liver.1 The methyl capping of all free hydroxyl groups (as in Pterostilbene) results in dramatically higher hepatic metabolic stability, intestinal absorption and membrane transport compared to unmethylated Resveratrol.2,3 Quercitin, pterostilbene and resveratrol are synergistic antioxidants, with quercitin seemingly aiding in the absorption of resveratrol.*4
Stilbenols are polyphenolic compounds that have cell-protecting properties.5 For Resveratrol, this action has mostly been linked to growth and death regulatory pathways. Research published in 2008 also demonstrated RES’s contribution to the maintenance of genome stability. Pterostilbene and quercetin, structurally-related and naturally-occurring, small polyphenols, show longer half-life in vivo than unmethylated resveratrol and have been shown to work synergistically to protect cellular health.*6
As exciting as its role in chemoprotection, is resveratrol’s ability to produce changes associated with longevity. These include increased insulin sensitivity, reduced IGF-1, increased AMP-activated protein kinase and peroxisome proliferator-activated receptor-gamma coactivator 1 alpha activity, increased mitochondrial number and improved motor function. Resveratrol opposed the effects of the high calorie diet in 144 of 153 significantly altered gene pathways.7 Resveratrol activates sirtuins including SIRT2, a special longevity cellular8 and SIRT1 that helps protect nerve cells.*9
In vitro, ex vivo and animal experiments have shown that the attributes of Resveratrol such as its powerful antioxidant activity, modulation of hepatic apolipoprotein and lipid synthesis, inhibition of platelet aggregation, and inhibition of human platelet and neutrophil production of pro-atherogenic eicosanoids favor protection against atherosclerosis.*10
Resveratrol’s numerous anti-inflammatory properties may explain why it has so many far-reaching health benefits. It inhibits synthesis and release of pro-inflammatory mediators, modifies eicosanoid synthesis, and inhibits activated immune cells. By inhibiting either NF-(kappa)B or the activator protein-1 (AP-1), resveratrol also appears to inhibit inducible nitric oxide synthase (iNOS) and cyclooxygenase-2 (COX-2).11 Specific human dosing to support a healthy inflammatory response has not yet been established.*
References
Wenzel E, Somoza V. Metabolism and bioavailability of trans-resveratrol. Mol [PMID:15779070]
Walle T, et al. High absorption but very low bioavailability of oral resveratrol in humans. DrugMetabDispos. 2004 Dec;32(12):1377-82. [PMID:15333514]
Wen X, Walle T. Methylated flavonoids have greatly improved intestinal absorption and metabolic stability. DrugMetabDispos. 2006 Oct;34(10):1786- 92 [PMID: 16868069]
Morimitsu Y, Sugihara N, Furuno K. Inhibitory effect of flavonoids on sulfo- and glucurono-conjugation of acetaminophen in rat cultured hepatocytes and liver subcellular preparations. BiolPharmBull. 2004 May;27(5):714-7. [PMID: 15133252]
Fresco P, Borges F, Diniz C, Marques MP. New insights on the anticancer properties of dietary polyphenols. MedResRev. 2006 Nov;26(6):747-66 [PMID: 16710860]
Ferrer P, et al.Association between pterostilbene and quercetin inhibits metastatic activity of B16 melanoma. Neoplasia. 2005 Jan;7(1):37-47. [PMID:15736313]
Baur JA, et al. Resveratrol improves health and survival of mice on a high- calorie diet. Nature. 2006 Nov; 16;444(7117):337-42. [PMID: 17086191]
Stefani M, et al. The effect of resveratrol on a cell model of human aging. AnnNYAcadSci. 2007 Oct;1114:407-18. [PMID: 17804521]
Soleas GJ, Diamandis EP, Goldberg DM. Resveratrol: a molecule whose time has come? And gone? ClinBiochem. 1997 Mar;30(2):91-113 [PMID:9127691]
de la Lastra CA, Villegas I.Resveratrol as an anti-inflammatory and anti- aging agent: mechanisms and clinical implications. MolNutrFoodRes. 2005 May;49(5):405-30 [PMID:15832402]
Hougee S, Faber J, Sanders A, de Jong RB, van den Berg WB, Garssen J, Hoijer MA, Smit HF. Selective COX-2 inhibition by a Pterocarpus marsupium extract characterized by pterostilbene, and its activity in healthy human volunteers. PlantaMed. 2005 May;71(5):387-92. [PMID: 15931573]
Mayo Clinic conducted a meta-analysis of randomized controlled trials (RCTs) testing the effects of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) on coronary heart disease (CHD). The goal was to evaluate improvement in patients taking these 2 Omega-3 fatty acids. This sounds like it should be a good study. However, not everything is as it seems so lets dig in to this one and see if it pans out as they stated.
The title of the study was “A Meta-Analysis of Randomized Controlled Trials and Prospective Cohort Studies of Eicosapentaenoic and Docosahexaenoic Long-Chain Omega-3 Fatty Acids and Coronary Heart Disease Risk.”
The investigators searched medical literature databases including Ovid/Medline, PubMed, Embase, and the Cochrane Library for studies regarding EPA & DHA, either from food or from supplements associated with cardiovascular disease (myocardial infarction, sudden cardiac death, coronary death, and angina). They looked at studies from 1947 to 2015 and identified 18 randomized controlled trials (RCTs) & 16 prospective cohort studies.
They wanted to evaluate the association of Omega-3 intake with coronary heart disease (CHD). They also wanted to evaluate the effect of the dose of Omega-3s as well as the effect of EPA & DHA on specific outcomes such as heart attacks (myocardial infarction). Each identified study was required to report at least one of the following: myocardial infarction (heart attack – fatal or non-fatal), chest pain (angina), sudden cardiac death, & CHD incidence. The studies had to include outpatient adults at least 18 years of age with or without CHD. They grouped the studies based on Omega-3 intake levels of below 1 gram per day or above 1 gram per day.
There were 93,000 participants in the RCT data and 732,000 participants in the prospective cohort data. There were 2 trials for primary prevention (preventing a first CHD event) with 27,494 participants. There were 9 trials focusing on mixed prevention and 12 trials focusing on secondary prevention.
One of the problems with meta-analysis as a study type is that your conclusions are only as good as the studies in the meta-analysis. The problem here is that there is a very wide range of Omega-3 dosing (0.38 grams to 23.8 grams per day for the primary and mixed prevention groups). It is likely that beneficial effects of Omega-3s were not noticed in the trial where they only took 380mg of EPA+DHA (0.38 grams) daily. Conversely, 23.8 grams per day is quite a lot.
The authors of the trial did observe that higher doses of EPA+DHA had a “stronger impact” in those with elevated triglyceride levels compared to trials where the participants took less than 1 gram per day of EPA+DHA.
Prospective cohort trials did demonstrate statistically significant reductions in CHD. The number is the percentage reduction for that event in patients taking Omega-3s.
Any CHD event – 18%
Fatal CHD events – 23%
Coronary death – 18%
Sudden cardiac death – 47%
They noted that Omega-3s reduced triglycerides as well as reduced risk of CHD in patients with LDL cholesterol >130. They felt that the benefit in regards to LDL may have been due to the change in LDL to the larger LDL particle which is less atherogenic. They also stated that “Blood pressure is another well-documented CHD risk factor impacted favorably by n-3 LCPUFA administration.”
Their conclusion?
“Results indicate that EPA+DHA may be associated with reducing CHD risk, with a greater benefit observed among higher-risk populations in RCTs.” However, I believe that further review of their data demonstrates that their conclusion statement is understating the effect of Omega-3s.
For example, one of the studies was a food recall questionnaire asking participants how many servings of fish they ate on a weekly basis. The investigators then assigned an Omega-3 quantity based on what type of fish meat it was (dark meat fish, canned tuna, and other fish). One confounding factor noted was that there was an inverse relationship of fish intake and red/processed meats. In other words, those that ate more fish ate less red/processed meats. It should be noted that there is a huge potential for bias in a food/diet recall questionnaire. Regardless, the investigators stated “In this prospective cohort study of diabetic women, higher consumption of fish and ω-3 fatty acids was associated with a lower incidence of both CHD and total mortality, even after adjustment for established cardiovascular risk factors.”2
Here are some of the studies evaluated in the Mayo Clinic Omega-3 Study
The DART Trial3
Another trial was merely based on whether or not they received dietary recommendations. 2033 male participants who had recovered from a heart attack (myocardial infarction) were randomized to either receive or not receive dietary advice. If they did receive dietary advice it was in regards to one of 3 groups: reduced fat intake (and increase in ratio of polyunsaturated fat to saturated fat), increase the amount of dietary fatty fish, or increase the amount of cereal fiber. The investigators noted that “The subjects advised to eat fatty fish had a 29% reduction in 2 year all-cause mortality compared with those not so advised.”3 I have several issues with relying on this study. There may be a good correlation with dietary advice regarding fish intake and coronary heart disease but there is no way to confirm how much fish they ate, their Omega-3 Index levels, quality of fish, etc.
GISSI-Prevenzione Trial4
This trial consisted of 11,324 participants who had survived a recent heart attack. They were randomized to receive Vitamin E (alpha-tocopherol, 300mg daily), Omega-3 supplements (1 gram daily), both of these, or neither of these for 3-5 years. The investigators wanted to evaluate if these supplements made a difference in death, non-fatal heart attack (myocardial infarction), or stroke.
They discovered that vitamin E supplementation did not make a difference. However, Omega-3 supplementation did with a relative risk reduction of 15% by 4-way analysis. The results for the group taking Vitamin E and Omega-3 combined were similar to those taking Omega-3s alone.
The ORIGIN Trial5
This study is very interesting because they showed that “Daily supplementation with 1 g of n–3 fatty acids did not reduce the rate of cardiovascular events in patients at high risk for cardiovascular events.” 12,536 participants were randomized to receive 900mg of ethyl ester Omega-3 (EPA 465 mg and DHA 375 mg) or a placebo. The participants had impaired fasting glucose, impaired glucose tolerance, or diabetes. They also received ither insulin glargine or standard care. Their primary outcome measurement was death from cardiovascular disease.
Why did this study not show improvement with Omega-3s when so many other studies do show improvement? The answer is simple. Their placebo was 1 gram of olive oil which is well known to have cardiovascular disease protective benefits!
The JELIS Trial6
There were 18,645 Japanese participants with a total cholesterol level of 251 mg/dL or more who were randomized to receive a statin only or a combination of a statin plus EPA 1800mg. Primary endpoints were any major adverse coronary events (sudden cardiac death, heart attacks, unstable angina, angioplasty, stents, or coronary artery bypass grafting [CABG]).
There was a 19% reduction in these Major Adverse Coronary Events (MACE) in the EPA + statin group at the end of 4-6 years. This study shows that patients have lower risk of cardiovascular disease outcomes if they are on EPA in addition to a statin.
The OMEGA Trial7
The OMEGA trial was a multicenter trial in Germany and consisted of 3,851 participants. It was a randomized, placebo-controlled, double-blinded (RCDBT) trial. Participants were randomized between 3 & 14 days after a heart attack to receive either 1 g omega-3 ethyl esters (EPA 460 mg & DHA 380 mg) or a soft gelatin capsule containing 1 g olive oil. This is yet another trial using olive oil as a placebo inappropriately. Therefore, they didn’t notice any difference between the 2 groups.
Coenzyme Q10 (CoQ10) is a fat-soluble substance that plays a major role in energy production and antioxidant protection in the body. It is found in the body primarily in its interchangeable ubiquinone and ubiquinol forms.
In general, CoQ10 supports mitochondrial energy production, antioxidant activity, cell membrane stabilization, gene expression and apoptosis, and neurological and cardiovascular health.1,2
Levels of CoQ10 in the body can be affected by a number of factors. Dietary contribution (through typical nutrition) of CoQ10 is minimal and serum levels tend to decline with age or can be reduced due to drug-induced nutrient depletion.*3-5
Synthesis of CoQ10 in the body is regulated by the enzyme HMG-CoA reductase. This is enzyme is the rate limiting step for the synthesis of cholesterol and is the target of statin medications. So, when you take a statin to decrease your cholesterol you also decrease the production of CoQ10. This is why EVERY patient taking a statin MUST be on a CoQ10 supplement!
A variety of factors can inhibit HMG-CoA reductase and hinder CoQ10 production and availability, resulting in a potential increase in oxidative stress and a decrease in energy generation.
In the event of reduced production, or drug-induced nutrient depletion, physicians recommend supplementation with CoQ10 to help maintain normal levels in the body.6,7 Supplementation with CoQ10 promotes favorable outcomes for a targeted group of patients8 and to improve quality of life, energy levels, neurological health maintenance, exercise tolerance, and muscle comfort for a wide range of individuals.1,9
A research study utilizing functional intracellular assay (Spectracell) suggested that CoQ10 may be a potential peripheral biomarker of antioxidant status in neurological health maintenance.*10
Cardiovascular health is particularly dependent upon CoQ10 because of the heart muscle’s exceedingly high energy demand.3 The value of CoQ10 supplementation on cardiovascular health has been confirmed by ongoing human research studies.6,11-13
A randomized, double-blind, placebo-controlled study utilizing the same bioidentical, naturally yeast-fermented CoQ10 found in Revolution’s CoQ10 formulas was conducted in a select group of 49 patients. Researchers observed that supplementation with 100 mg/d of CoQ10 successfully restored plasma levels and significantly increased total CoQ10 levels by 127%.*14
Results from the highly anticipated Q-SYMBIO research study were reported in May 2013. Prior to the Q-SYMBIO study, researchers had observed that myocardial CoQ10 levels were inversely related to heart health and function.15 The Q-SYMBIO results, in fact, supported this association.
In the randomized, double-blind, placebo controlled Q-SYMBIO study, 420 patients were assigned to parallel groups to receive either the CoQ10 found in CoQ10-ME (100 mg three times per day) or placebo. Within three months, researchers observed a reduction in N-terminal pro-brain natriuretic peptide (NT-proBNP), an important marker of heart health, in the CoQ10 supplemented patients. After two years, patients who were supplemented with CoQ10 had significant cardiovascular improvement overall compared to placebo.*16,17
CoQ10 has the following benefits: improves endothelial & mitochondrial function; protects against LDL oxidation; lowers ICAM & IL-6; increases HDL-C; improves angina, CHD, CHF, ventricular arrhythmias, reverses statin induced diastolic dysfunction, reduces MACE 43% & all cause mortality 50% (Q-SYMBIO trial).
Revolution’s CoQ10 contains a unique, crystal-free, highly bioavailable form of ubiquinone and represent a new generation of CoQ10 supplementation. This soy-free formulation contains five lipids that help dissolve CoQ10 crystals into single molecules. This process helps stabilize the formula to prevent re-crystallization and facilitates passive diffusion to enhance absorption.
Earlier generation supplements were poorly absorbed (0.6-1.0%), pure crystalline (powdered) forms of CoQ10, which served as the industry standard from the mid-1970s to the mid-1990s. A variety of forms and delivery systems offered somewhat improved absorption (2.3-5%) after 1995.
However, these forms were unstable and crystallized and therefore difficult for the body to absorb. The five-lipid carrier, crystal-free CoQ10 in Revolution’s CoQ10-ME represents innovation and improvement in CoQ10 delivery and bioavailability.*
Goal: Serum levels should be >3mcg/mL. However, serum testing may be unreliable as it may not reflect intracellular levels due to transmembrane gradients.
Dose: Start with 1 capsule daily. We adjust your dose according to your serum testing as well as the Spectracell test.
References:
Morris G, Anderson G, Berk M, et al. Coenzyme Q10 Depletion in Medical and Neuropsychiatric Disorders: Potential Repercussions and Therapeutic Implications. Mol Neurobiol. 2013 Jun 13. [Epub ahead of print] [PMID: 23761046]
Higdon J. CoQ10. Linus Pauling Institute. http://lpi.oregonstate.edu/infocenter/othernuts/ coq10/. February 2003. Updated March 2012. Accessed July 25, 2013.
Berthold HK, Naini A, Di Mauro S, et al. Effect of ezetimibe and/or simvastatin on coenzyme Q10 levels in plasma: a randomised trial. Drug Saf. 2006;29(8):703-12. [PMID: 16872244]
Rundek T, Naini A, Sacco R, et al. Atorvastatin decreases the coenzyme Q10 level in the blood of patients at risk for cardiovascular disease and stroke. Arch Neurol. 2004 Jun;61(6):889-92. [PMID: 15210526]
Langsjoen PH, Langsjoen AM. The clinical use of HMG CoA-reductase inhibitors and the associated depletion of coenzyme Q10. A review of animal and human publications. Biofactors. 2003;18(1-4):101-11. Review. [PMID: 14695925]
Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr. 2001 Dec;20(6):591-8. Review. [PMID: 11771674]
Potgieter M, Pretorius E, Pepper MS. Primary and secondary coenzyme Q10 deficiency: the role of therapeutic supplementation. Nutr Rev. 2013 Mar;71(3):180-8. [PMID: 23452285]
Zlatohlavek L, Vrablik M, Grauova B, et al. The effect of coenzyme Q10 in statin myopathy. Neuro Endocrinol Lett. 2012;33 Suppl 2:98-101. [PMID: 23183519]
Mischley LK, Allen J, Bradley R. Coenzyme Q10 deficiency in patients with Parkinson’s disease. J Neurol Sci. 2012 Jul 15;318(1-2):72-5. [PMID: 22542608]
Littarru GP, Tiano L. Clinical aspects of coenzyme Q10: an update. Curr Opin Clin Nutr Metab Care. 2005 Nov;8(6):641-6. Review. [PMID: 16205466]
Munkholm H, Hansen HH, Rasmussen K. Coenzyme Q10 treatment in serious heart failure. Biofactors. 1999;9(2-4):285-9. [PMID: 10416042]
Fotino AD, Thompson-Paul AM, Bazzano LA. Effect of coenzyme Q10 supplementation on heart failure: a meta-analysis. Am J Clin Nutr. 2013 Feb;97(2):268-75. [PMID: 23221577]
Mabuchi H, Nohara A, Kobayashi J, et al. Effects of CoQ10 supplementation on plasma lipoprotein lipid, CoQ10 and liver and muscle enzyme levels in hypercholesterolemic patients treated with atorvastatin: a randomized double-blind study. Atherosclerosis. 2007 Dec;195(2):e182-89. [PMID: 17681347]
Folkers K, Vadhanavikit S, Mortensen SA. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc Natl Acad Sci U S A. 1985 Feb;82(3):901-4. [PMID: 3856239]
Mortensen SA, Kumar A, Dolliner P, et al. The effect of Coenzyme Q10 on morbidity and mortality in chronic heart failure. Results from the Q-SYMBIO study. [ESCARDIO abstract 440]. European Journal of Heart Failure. 2013 15(S1):S20. http://spo.escardio.org/ SessionDetails.aspx?eevtid=61&fp=440&doc=abstract#.UfQgDI2TjSg. Accessed July 25, 2013.
European Society of Cardiology. Important new data shows CoQ10 improves survival in heart failure patients. http://www.escardio.org/congresses/hf2013/congress-to-you/Pages/ new-data-CoQ10-improves-survival-heart-failure-patients.aspx. Accessed July 28, 2013.
When it comes to nutritional supplements we have to address both of these.
Are you tired of guessing when it comes to your nutrition?
Are you spending money on supplements you don’t need?
We have the solution for you!
Quality in nutritional supplements is our first priority. Many of our patients ask for a thorough nutritional evaluation. Spectracell offers a great test that evaluates the functional status of your physiology based on your nutrient status.
Chromium is an essential trace mineral that plays an important role in optimizing insulin function and the regulation of blood glucose levels. Chromium may also be anti-atherogenic and assist in lowering cholesterol. Following food intake, blood glucose levels rise causing insulin to be secreted by the pancreas. Insulin lowers blood glucose levels by increasing the rate at which glucose enters a person’s cells. Chromium is believed to facilitate the attachment of insulin to the cell’s insulin receptors. Studies also indicate that chromium participates in cholesterol metabolism, suggesting a role for this mineral in maintaining normal blood cholesterol levels and preventing atherosclerosis. Chromium also plays a role in nucleic acid synthesis.
Deficiency Symptoms:
Due to processing methods that remove most of the naturally occurring chromium from commonly consumed foods, dietary deficiency of chromium is believed to be widespread in the United States. Chromium deficiency may increase the likelihood of insulin resistance, a condition which the cells of the body do not respond to the presence of insulin. Insulin resistance an lead to elevated blood levels of insulin (hyperinsulinemia) and elevated blood levels of glucose, which can ultimately cause heart disease and/or diabetes. Deficiency of chromium is associated with metabolic syndrome. Metabolic syndrome represents a constellation of symptoms, including hyperinsulinemia, high blood pressure, high triglyceride levels, high blood sugar levels, and low HDL cholesterol levels. These symptoms increase one’s risk for heart disease. Low levels of chromium are also associated with an increased risk of coronary artery disease incidence and mortality.
Chromium deficiency correlate with depressed nucleic acid synthesis. Chromium is essential for maintaining the structural stability of proteins and nucelic acids and animal studies have found that this element is also vital for healthy fetal growth and development. Studies on humans have established that premature infants and those with evidence of intrauterine growth retardation have significantly lower chromium status compared to infants born full-term. Others have found that multiparous women have far lower body chromium levels compared to nulliparous women. These findings suggest that chromium is an essential trace element during fetal growth and development.
Repletion Information:
In 2001, the Institute of Medicine at the National academy of Sciences conducted a thorough review of the chromium research can concluded that excessive intake of chromium from foods or supplements is not associated with any adverse effects. As a result, to Tolerable Upper Intake Level (UIL) was established for this mineral. However, people with liver or kidney disease may be more susceptible to adverse effects from excessive intake of chromium, and such individuals are cautioned to avoid taking more than 200 micrograms of chromium supplements per day. There is limited evidence to suggest that long-term chromium picolinate supplementation at levels greater than 200 micrograms per day may also be hazardous to chromosome integrity and should be avoided.
We deal with Glutathione in our clinic in Tulsa Functional Medicine Clinic frequently. Why? What is glutathione and what does it do?
Reduced glutathione, commonly known as glutathione or GSH, is a tripeptide (3 amino acids) consisting of L-glutamine, L-cysteine, and glycine. It is ubiquitous in living systems.
Glutathione biosynthesis can be affected by biochemical individuality and/or dietary factors. Chronic oxidative stress can also deplete cellular glutathione. Precursors to glutathione, such as whey protein, vitamin C, and glutamine, are often recommended to boost glutathione levels in the body; however, results are inconsistent.
Biological individuality is such that not every body has equivalent ability to metabolize the precursors to raise glutathione.*
Glutathione has numerous cellular function benefits including antioxidant protection and detoxification. It is essential for the maintenance of cell membrane integrity in red blood cells.
Intracellular glutathione concentrations (as determined by the Spectracell test) are principally derived by intracellular synthesis, as few cells directly uptake glutathione from the surrounding extracellular fluid. The high concentration of glutathione in virtually all cells clearly indicates its importance in metabolic and oxidative detoxification processes.
Glutathione is considered the “Master Antioxidant.”
Deficiency Symptoms
A wide range of human conditions such as aging, cancer, atherosclerosis, arthritis, viral infections, AIDS, cardiovascular, neurodegenerative diseases and pulmonary diseases may be produced, or made worse, by “free radicals.”
The treatment or prevention of these conditions often includes antiooxidants such as Vitamin C, Vitamin E, carotenoids, and selenium. Glutathione is an essential component of the antioxidant defense system producing a “sparing effect” for both tocopherol and ascorbate by reducing the oxidized forms, and by eliminating hydrogen peroxide by reacting with glutathione peroxidase.
Cellular glutathione functions to decrease the formation of oxidized LDL, implicated in the development of atherosclerosis. T-lymphocytes become deficient in glutathione in the prostaglandins from n-3 and n-6 polyunsaturated fatty acids which are important in the inflammatory response.
Patients with adult respiratory distress syndrome are favorably affected by treatments that increase cellular glutathione.
Why Not Give Pure Glutathione?
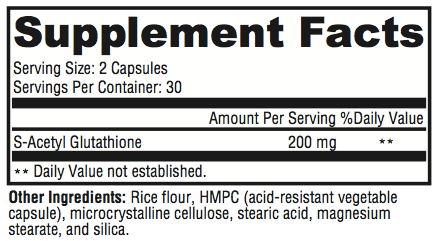
Glutathione is poorly absorbed from the GI tract and foods rich in glutathione do not appear to contribute to increases in intracellular glutathione levels.
Unfortunately, most oral forms of glutathione are foul smelling, but more importantly, the majority of an oral dose is oxidized before it can be absorbed and used by the cells. This formulation delivers a unique preparation of glutathione that overcomes these usual limitations. The stability of S-acetyl glutathione through the intestinal wall and the plasma is well documented in the literature. Oral intake of S-acetyl glutathione increases total glutathione and percent-reduced glutathione. Percent-reduced glutathione is a very significant biomarker of health status.*[1-5]
Cysteine appears to be the limiting amino acid in the intracellular synthesis of glutathione and supplementation with up to 2000mg daily of N-Acetyl Cysteine appears safe.
Supplementation with normal cysteine is not recommended as it may be poorly tolerated by many patients. In addition, it may be rapidly oxidized to L-cystine, a less usable form for the synthesis of glutathione. Foods rich in cysteine are generally high protein foods such as meats, yogurt, wheat germ, and eggs.
Mechanism of Absorption
S-acetyl glutathione, a lipid-like compound, is taken up intact by chylomicrons in the gut. The acetyl bond is placed on its thiol group or sulfur group, which prevents oxidation and allows the molecule to pass diffusively into the cell after absorption in the gut.
The acetyl bond is then cleaved by non-specific enzymes inside the cell. Acetylation prevents the breakdown of glutathione, and S-acetyl glutathione does not require energy expenditure to be cleaved to reduced glutathione once it crosses the cell wall.*1-8
Antioxidant Activity
Glutathione functions extensively in tissues and organs throughout the body. It plays critical roles in protecting the body from oxidative stress, maintaining cellular functions, and supporting healthy immune function.1,4
Many factors can increase cellular exposure to oxidative insult, and therefore increase cellular consumption of nutrients—such as glutathione—that provide antioxidant activity. This may result in a fierce cycle of oxidative stress and challenges to detoxification. Complete biotransformation and protection from oxidative stress are important to maintaining cellular integrity and tissue health.*2,5
Other Benefits of Maintaining Healthy Glutathione Levels
Much information related to mitochondrial health has surfaced in the literature. Mitochondria, the energy-producing powerhouses of cells, are also the primary intracellular site of oxygen consumption and the major source of reactive oxygen species (ROS). S-acetyl glutathione has been shown to cross the membrane of the mitochondria, increasing the organelle’s activity and minimizing ROS.8,9 Reduction of ROS is associated with maintaining mitochondrial integrity and function, and improved mitochondrial health is believed to support overall health and energy.*
S-acetyl glutathione has also been shown to decrease TNF-alpha, NF-kappa beta, and F-2 isoprostane.4,9-12 Additionally, there is mounting evidence that intracellular glutathione levels in antigen-presenting cells (e.g. macrophages) may influence the Th1/Th2 cytokine response pattern and promote a balanced immune reaction.*10
Directions
Take 2 capsules daily for general support and therapy. For Alzheimer’s prophylaxis, take 1 capsule daily.
References
Locigno R, Pincemail J, Henno A, et al. S-Acetyl-glutathione selectively induces apoptosis in human lymphoma cells through a GSH- independent mechanism. Int J Oncol. 2002 Jan;20(1):69-75. [PMID: 11743644]
Lomaestro BM, Malone M. Glutathione in health and disease: pharmacotherapeutic issues. Ann Pharmacother. 1995 Dec;29(12):1263-73. [PMID: 8672832]
Cacciatore I, Cornacchia C, Pinnen F, et al. Prodrug approach for increasing cellular glutathione levels. Molecules. 2010 Mar 3;15(3):1242- 64. [PMID: 20335977]
Vogel J, Cinatl J, Dauletbaev N, et al. Effects of S-acetylglutathione in cell and animal model of herpes simplex virus type 1 infection. Med Microbiol Immunol. 2005 Jan;194(1-2):55-59. [PMID: 14624358]
Ballatori N, Krance SM, Notenboom S, et al. Glutathione dysregulation and the etiology and progression of human diseases. Biol Chem. 2009 Mar;390(3):191-214. [PMID: 19166318]
Richman PG, Meister A. Regulation of gamma-glutamyl-cysteine synthetase by nonallosteric feedback inhibition by glutathione. J Biol Chem. 1975 Feb 25;250(4):1422-26. [PMID: 1112810]
Anderson ME, Powrie F, Puri RN, et al. Glutathione monoethyl ester: preparation, uptake by tissues, and conversion to glutathione. Arch Biochem Biophys. 1985 Jun;239(2):538-48. [PMID: 4004275]
Anderson ME, Nilsson M, Sims NR. Glutathione monoethyl ester prevents mitochondrial glutathione depletion during focal cerebral ischemia. Neurochem Int. 2004 Feb;44(3):153-59. [PMID: 14568558]
Kretzschmar M. Regulation of hepatic glutathione metabolism and its role in hepatotoxicity. Exp Toxicol Pathol. 1996 Jul;48(5):439-46. [PMID: 8765689]
Fraternale A, Paoletti MF, Casabianca A, et al. Antiviral and immunomodulatory properties of new pro-glutathione (GSH) molecules. Curr Med Chem. 2006;13(15):1749-55. [PMID: 16787218]
Kretzschmar M, Klinger W. The hepatic glutathione system—influences of xenobiotics. Exp Pathol. 1990;38(3):145-64. [PMID: 2192911]
Donnerstag B, Ohlenschlager G, Cinatl J, et al. Reduced glutathione and S-acetylglutathione as selective apoptosis-inducing agents in cancer therapy. Cancer Lett. 1996 Dec;110(1-2):63-70. [PMID: 9018082]
It is rare that people get adequate nutrition with the food we eat today. Most foods are not of the quality that we ate just a few decades ago and the impact can be severe. We test many of our patients with a comprehensive micronutrient test which helps us thoroughly evaluate each individual patient’s nutrition and nearly all of them are deficient in at least 1 nutrient and most are deficient in several.
One of the tenants of the Healthy Trinity is nutrition and it is a critical component of optimal health. We find that most patients need nutritional supplements on some level. Additionally, most of our patients have medical conditions that are most appropriately treated with nutritional supplements.
One problem with supplements is that the quality can vary dramatically. Consumer Reports ran tests on some common & well-known brands of supplements and the results were quite disappointing. 30% of the supplements tested did not contain what their label stated. More concerning, some of them were contaminated with lead – up to 26 times the amount allowed by ConsumerLabs. 66% of the multivitamins that were tested failed. The poor quality and contamination give great concern for some nutritional supplements.
So how do you know what brand you can trust? It is easier than you think! Look for a brand that performs independent, 3rd-party testing. That means they voluntarily send their supplements to the lab to have them tested. Most companies don’t do this because it is expensive. We had a hard time finding a manufacturer that did this type of testing.
Revolution’s supplements are independently 3rd-party tested
We have the kind of quality that you want and deserve. It is the kind of quality you can feel safe in taking for yourself or giving to your kids.
Our supplements are pharmaceutical grade and physician formulated. They are backed by human clinical trials documenting their effects.
Pantothenic Acid (as d-calcium pantothenate) Pantothenic acid, a B complex vitamin also known as vitamin B5, occurs as an unstable oil. Its water-soluble salt, d-calcium pantothenate, is the form most commonly used in supplements. D-calcium pantothenate is composed of 91.5% pantothenic acid and 7.5% calcium. Among its many physiological functions, pantothenic acid is a precursor to the synthesis of coenzyme A (CoA), is an essential cofactor for ATP production, and is essential to the adrenal cortex for production of glucocorticoids.*
Vitamin B6 (as pyridoxal 5’-phosphate and pyridoxine HCl) Corticare BTM provides vitamin B6 as both pyridoxine HCl and activated pyridoxal 5’-phosphate, the form in which B6 is transported in the blood. Physiologically, vitamin B6 influences the adrenal glucocorticoid receptor, stimulates the secretion of adrenal catecholamines, and aids in sodium and potassium balance.*
Vitamin C (as magnesium ascorbate) The release of adrenocorticotropic hormone (ACTH) from the pituitary gland in tandem with the body’s physiological response to stress will deplete the relatively large amount of vitamin C typically stored in the adrenal cortex. This vitamin is essential for the synthesis of epinephrine, the hormone secreted by the adrenal medulla in response to stress. Epinephrine, in turn, plays a role in the synthesis of aldosterone, the hormone that regulates blood pressure, volume, and pH.*
Folate (as calcium folinate and 5-MTHF) Corticare B provides the activated form of folic acid—5-MTHF as Quatrefolic—to ensure superior bioavailability. Folic acid is important for building and repairing protein that may be broken down by stress hormones. It is also key to the synthesis of serotonin, a neurotransmitter that affects mood, appetite, and sleep, all of which are often negatively affected by stress.*
L- Carnitine (as tartrate) This conditionally essential nutrient derived from lysine is needed for the “carnitine shuttle.” It transports long- chain fatty acyl CoA from the outside to the inside of the mitochondria, making it a key nutrient in the production of energy.*
BioPerine® This patented extract of black pepper (Piper nigra) has been shown to significantly enhance the availability of vitamin C and vitamin B6.*
Directions:
Take two capsules daily, or as directed by your healthcare practitioner.
Quatrefolic ® – The fourth generation folate. www.quatrefolic.com. Accessed July 12, 2011.
Miller AL. The methylation, neurotransmitter, and antioxidant connections between folate and depression. Altern Med Rev. 2008 Sep;13(3):216-26. [PMID: 18950248]
Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl 1):12-6. [PMID: 16001092]
BioPerine® – An Ingredient of Sabinsa. www.bioperine.com. Updated April 20, 2010. Accessed July 12, 2011.
CoQ10 and the CoQ10 cycle play fundamental roles in the antioxidant and energy systems of the body. The ubiquinone form of CoQ10 is produced in the mitochondria, where it directly participates in energy production by accepting electrons in the electron transport chain. Through the action of an oxidoreductase enzyme, ubiquinone is rapidly converted to ubiquinol, the lipid- soluble form that supports antioxidant activity throughout the body. Conversion of ubiquinone to ubiquinol declines with age, particularly after age 40.
Supplementation may help maintain normal levels of ubiquinol in the body as well as address drug-induced nutrient depletion of CoQ10. Until recently, the ubiquinol form had not been effective as a supplement because it was chemically unstable and easily oxidized.
AntioxidantStatus Oxidative stress is detrimental to the integrity and function of cell membranes and tissues, and ultimately to DNA itself. Antioxidant status must be maintained throughout the body in order to protect vulnerable cells. Research indicates that CoQ10 supports antioxidant activity, including the regeneration of vitamins C and E, helping to maintain normal levels of free radical activity in the body. Researchers also suggest a possible role for CoQ10 in redox control of cell signaling and gene expression.*
Cholesterol Antioxidant protection is vital to maintaining the integrity of cholesterol and its role as a precursor to vitamin D, hormones, cell membranes, and brain tissue. Reactive oxygen species, including superoxide released by immune cells, cause the oxidation of cholesterol and can turn a vital biochemical precursor into a toxin.*
CoQ10Depletion Serum CoQ10 levels decline with age but are
also reduced with inhibition of the HMG-CoA reductase enzyme,
an enzyme essential to CoQ10 production. In the event of reduced production, or drug-induced nutrient depletion, supplementation with CoQ10 helps maintain normal levels in the body. Related depletion of vitamin E in lymphocytes may raise further concerns about patients’ vulnerability to oxidative stress.*
HeartHealth Research suggests that patients experienced significant support of cardiac function after receiving supplemental CoQ10 (an average 450-580 mg per day). These patients achieved more desirable levels of serum CoQ10 when switched from ubiquinone to ubiquinol. Researchers suggest that ubiquinol had dramatically improved absorption. Research on the elderly also appears to indicate that supplemental CoQ10 can increase tolerance to aerobic stress in cardiac tissue.*
Aging The role of CoQ10 in aging has become a topic of great interest. Supplementation with both forms of CoQ10—ubiquinone and ubiquinol—was studied in a SAMP1 mouse model. Results suggest that the ubiquinol form more effectively raised CoQ10 levels in the liver (the main target tissue), followed by kidney, heart, and brain. Ubiquinol also appeared to have a more positive effect on maintenance of healthy function than did ubiquinone.*
KanekaQH Stabilized ubiquinol was developed by Kaneka Corporation (the world’s largest manufacturer of CoQ10) and was found to be safe and bioavailable following single and multiple doses.*
Directions:
Take one to two softgels daily, or as directed by your healthcare practitioner.
References:
Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr. 2001 Dec;20(6):591-8. Review. [PMID: 11771674]
Cathcart MK, McNally AK, Morel DW, et al. Superoxide anion participation in human monocyte-mediated oxidation of low-density lipoprotein and conversion of low-density lipoprotein to a cytotoxin. J Immunol. 1989 Mar 15;142(6):1963- 9. [PMID: 2537865]
Langsjoen PH, Langsjoen AM. The clinical use of HMG CoA-reductase inhibitors and the associated depletion of coenzyme Q10. A review of animal and human publications. Biofactors. 2003;18(1-4):101-11. Review. [PMID: 14695925]
Passi S, Stancato A, Aleo E, et al. Statins lower plasma and lymphocyte ubiquinol/ubiquinone without affecting other antioxidants and PUFA. Biofactors. 2003;18(1-4):113-24. [PMID: 14695926]
Langsjoen PH, Langsjoen AM. Supplemental ubiquinol in patients with advanced congestive heart failure. Biofactors. 2008;32(1-4):119-28. [PMID: 19096107]
Rosenfeldt FL, Pepe S, Ou R, t al. Coenzyme Q10 improves the tolerance of the senescent myocardium to aerobic and ischemic stress: studies in rats and in human atrial tissue. Biofactors. 1999;9(2-4):291-9. [PMID: 10416043]
Schmelzer C, Kubo H, Mori M, et al. Supplementation with the reduced form of Coenzyme Q10 decelerates phenotypic characteristics of senescence and induces a peroxisome proliferator-activated receptor-alpha gene expression signature in SAMP1 mice. Mol Nutr Food Res. 2010 Jun;54(6):805-15. [PMID: 19960455]
Yan J, Fujii K, Yao J, et al. Reduced coenzyme Q10 supplementation decelerates senescence in SAMP1 mice. Exp Gerontol. 2006 Feb;41(2):130-40. [PMID: 16387461]
Kaneka QHTM Ubiquinol. http://www.kanekaqh.com. Accessed December 15, 2011.
Hosoe K, Kitano M, Kishida H, et al. Study on safety and bioavailability of ubiquinol (Kaneka QH) after single and 4-week multiple oral administration to healthy volunteers. Regul Toxicol Pharmacol. 2007 Feb;47(1):19-28. [PMID: 16919858]
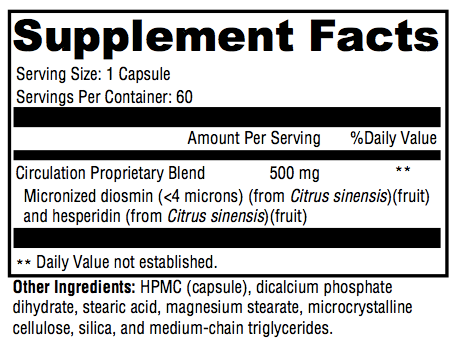
Diosmin is a well-researched citrus flavonoid that has been utilized for decades to support healthy capillary and vein function as well as healthy microcirculation throughout the body. Diosmin fundamentally helps maintain the structure and function of the circulatory system, especially vein strength and competence. The most promising research results come from a micronized purified flavonoid fraction comprising 450 mg of diosmin and 50 mg of hesperidin (hesperidin is a precursor to diosmin). This is the same ratio and dose found in each DioVasc capsule. The process of micronization (reducing particle size to less than two micrometers in diameter) improves diosmin absorption.*
Micronized purified flavonoid fraction (MPFF) appears to support vein health by prolonging the normal effect that the catecholamine norepinephrine has on the vessel wall; and this, therefore, promotes venous tone. Research also suggests that MPFF affects the synthesis of prostaglandins and free radicals, as well as leukocyte activation, trapping, and migration. Ultimately MPFF supports antioxidant systems and the body’s normal response to inflammation.*
Pharmacological and clinical studies suggest that MPFF—on its own and in conjunction with standard therapy—promotes normal lymph drainage, healthy capillary permeability, and favorable microcirculation. Multicenter, prospective, randomized, controlled studies document the effect of MPFF on maintaining healthy venous sufficiency. Two randomized, double-blind, placebo-controlled studies conducted over a two-month period demonstrated the venotropic nature of DioVasc’s main component. Significant support of organic and functional parameters occurred along with significant support of venous hemodynamics. Some studies indicate that favorable results can be achieved within two hours of administration.*
A review of the literature suggests that health-related quality-of-life parameters were found to improve with the use of MPFF and were associated with the formula’s support of microcirculation and vein function. A single-center, double-blind, placebo-controlled study suggested that MPFF had a positive and protective effect on five study variables (red blood cell aggregation, red blood count, microcirculatory blood flux, and amplitude and frequency of vasomotion). A double-blind placebo-controlled trial of MPFF over a six-week period suggested that the formula, administered twice daily, significantly (p <0.001) supported capillary structure and health and was well tolerated throughout the study. A double-blind randomized study of 104 subjects over a three-month period revealed that MPFF at various doses (500 mg, 1000 mg, or 2000 mg per day) significantly supported transcutaneous oxygen pressure and venous competence.*
A meta-analysis of five prospective, randomized, controlled studies employing a total of 723 subjects suggested that MPFF promoted healthy tissue integrity when combined with conventional therapy (compression and local care). Similar results were obtained in a multicenter, double-blind, randomized, controlled study of 107 individuals.*
The worldwide RELIEF program (Reflux assEssment and quaLity of lIfe improvEment with micronized Flavonoids) studied the effects of MPFF on more than 5000 participants in 23 countries. A variety of subjects taking MPFF over a six-month period showed clinically significant improvements that indicated MPFF’s supportive effect on microcirculation and vein health and function. These improvements continued throughout the study.*
Placebo-controlled human trials support the use of MPFF for the maintenance of healthy metabolic parameters, microcirculation, fluid balance, lymph system function, and albumin retention. Results suggest that MPFF specifically supports normal capillary filtration, lymphatic albumin resorption, and fluid balance at the cellular level. Research on MPFF suggests that its positive effects may be extended to various parts of the body.*
Ongoing animal studies suggest that diosmin, the major component found in MPFF, significantly supports blood glucose and insulin levels already within the normal range and exerts favorable effects on maintaining healthy serum hemoglobin. Researchers hope to apply these benefits to maintaining healthy metabolic parameters in humans as well.*
Directions:
Take one capsule twice daily, or as directed by your healthcare practitioner.
Children, pregnant or lactating women, and individuals using blood thinners should consult their healthcare practitioner prior to use. Do not use if tamper seal is damaged.
References:
Monograph. Diosmin. Altern Med Rev. 2004 Sep;9(3):308-11. [PMID: 15387721]
2. Lyseng-Williamson KA, Perry CM. Micronised purified flavonoid fraction: a review of its use in chronic venous insufficiency, venous ulcers and haemorrhoids. Drugs. 2003;63(1):71-100. [PMID: 12487623]
3. Pitsch F. Recent guidelines in chronic venous disease: the place of Daflon 500 mg. Phlebolymphology. 2011;18:24-29. http://www.phlebolymphology. org/2011/01/recent-guidelines-in-chronic-venous-disease-the-place-of-daflon-500-mg/. Accessed October 12, 2012.
4. Bergan JJ, Schmid-Schönbein GW, Takase S. Therapeutic approach to chronic venous insufficiency and its complications: place of Daflon 500 mg. Angiology. 2001 Aug;52 Suppl 1:S43-7. [ PMID: 11510596]
5. Smith PD. Neutrophil activation and mediators of inflammation in chronic venous insufficiency. J Vasc Res. 1999;36 Suppl 1:24-36. [PMID: 10474048]
6. Korthui RJ, Gute DC. Anti-inflammatory actions of a micronized, purified flavonoid fraction in ischemia/reperfusion. Adv Exp Med Biol. 2002;505:181-90. [PMID: 12083462]
7. Jean T, Bodinier MC. Mediators involved in inflammation: effects of Daflon 500 mg on their release. Angiology. 1994 Jun;45(6 Pt 2):554-9. [PMID: 8203787] 8. Ramelet AA. Clinical benefits of Daflon 500 mg in the most severe stages of chronic venous insufficiency. Angiology. 2001 Aug;52 Suppl 1:S49-56. [PMID: 11510597]
9. Laurent R, Gilly R, Frileux C. Clinical evaluation of a venotropic drug in man. Example of Daflon 500 mg. Int Angiol. 1988 Apr-Jun;7(2 Suppl):39-43. [PMID: 3053942]
10. Tsouderos Y. Are the phlebotonic properties shown in clinical pharmacology predictive of a therapeutic benefit in chronic venous insufficiency? Our experience with Daflon 500 mg. Int Angiol. 1989 Oct-Dec;8(4 Suppl):53-9. [PMID: 2698902]
11. Le Dévéhat C, Khodabandehlou T, Vimeux M, et al. Evaluation of haemorheological and microcirculatory disturbances in chronic venous insufficiency: activity of Daflon 500 mg. Int J Microcirc Clin Exp. 1997;17 Suppl 1:27-33. [PMID: 9477042]
12. Galley P, Thiollet M. A double-blind, placebo-controlled trial of a new veno-active flavonoid fraction (S 5682) in the treatment of symptomatic capillary fragility. Int Angiol. 1993 Mar;12(1):69-72. [PMID: 8376915]
13. Belcaro G, Cesarone MR, de Sanctis MT, et al. Laser Doppler and transcutaneous oximetry: modern investigations to assess drug efficacy in chronic venous insufficiency. Int J Microcirc Clin Exp. 1995;15 Suppl 1:45-9. [PMID: 8748889]
14. Coleridge-Smith P, Lok C, Ramelet AA. Venous leg ulcer: a meta-analysis of adjunctive therapy with micronized purified flavonoid fraction. Eur J Vasc Endovasc Surg. 2005 Aug;30(2):198-208. [PMID: 15936227]
15. Smith PC. Daflon 500 mg and venous leg ulcer: new results from a meta-analysis. Angiology. 2005 Sep-Oct;56 Suppl 1:S33-9. [PMID: 16193225]
16. Guilhou JJ, Dereure O, Marzin L, et al. Efficacy of Daflon 500 mg in venous leg ulcer healing: a double-blind, randomized, controlled versus placebo trial in 107 patients. Angiology. 1997 Jan;48(1):77-85. [PMID: 8995348]
17. Jantet G. Chronic venous insufficiency: worldwide results of the RELIEF study. Reflux assEssment and quaLity of lIfe improvEment with micronized Flavonoids. Angiology. 2002 May-Jun;53(3):245-56. [PMID: 12025911]
18. Valensi PE, Behar A, de Champvallins MM,et al. Effects of a purified micronized flavonoid fraction on capillary filtration in diabetic patients. Diabet Med. 1996 Oct;13(10):882-8. [PMID: 8911782]
19. Valensi P, Behar A. Clinical implications of impaired microcirculation. Int Angiol. 1995 Sep;14(3 Suppl 1):26-31. [PMID: 8919261]
20. Behar A, Valensi P, de Champvallins M, et al. Capillary filtration and lymphatic resorption in diabetes. Application to the pharmacodynamic activity of Daflon 500 mg. Int Angiol. 1989 Oct-Dec;8(4 Suppl):27-9. [PMID: 2632646]
21. Buckshee K, Takkar D, Aggarwal N. Micronized flavonoid therapy in internal hemorrhoids of pregnancy. Int J Gynaecol Obstet. 1997 May;57(2):145-51. [PMID: 9184951]
22. Cospite M. Double-blind, placebo-controlled evaluation of clinical activity and safety of Daflon 500 mg in the treatment of acute hemorrhoids. Angiology. 1994 Jun;45(6 Pt 2):566-73. [PMID: 8203789]
23. Pari L, Srinivasan S. Antihyperglycemic effect of diosmin on hepatic key enzymes of carbohydrate metabolism in streptozotocin-nicotinamide-induced diabetic rats. Biomed Pharmacother. 2010 Sep;64(7):477-81. [PMID: 20362409]
24. Srinivasan S, Pari L. Ameliorative effect of diosmin, a citrus flavonoid against streptozotocin-nicotinamide generated oxidative stress induced diabetic rats. Chem Biol Interact. 2012 Jan 5;195(1):43-51. [PMID: 22056647]
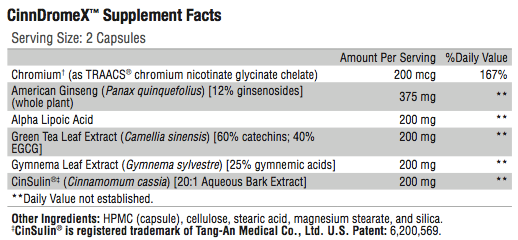
Cinnulin PFTM contains the bio-active, water-soluble polyphenol polymers (“Type-A polymers”) that inhibit PTP-1, preventing inactivation of insulin receptors. They affect protein phosphorylation- dephosphorylation reactions regulating glucose metabolism signal transduction pathways. These Polymers are antioxidants and increase insulin-dependent glucose metabolism by roughly 20 times. After 40 days of consuming either one, three or six grams of cinnamon per day, subjects had significant reductions in blood glucose (18-29%) and blood lipids (7-30%).*
AmericanGinseng (Panax quinquefolius) possesses sulfonylurea- like activity. This herb does not lower blood sugar unless it contains a significant quantity of ginsenosides. The American ginseng in CinnDromeXTM is a standardized 12% (ginsenosides) extract.*
Gymnema Leaf Extract (Gymnema sylvestre) is a water-soluble extract made from the leaves of Gymnema sylvestre and standardized to 25% gymnemic acid. This form does not decrease iron absorption as other forms may. Gymnema can enhance the effects of insulin and oral hypoglycemic agents by reducing glucose absorption in
the intestine, stimulating pancreatic beta cell growth and possibly increasing endogenous insulin secretion. Gymnema may also reduce serum lipids.*
Green Tea Polyphenols (Camelia sinesis) protect erythrocytes from oxidative stress, possibly reducing risk of late complications of diabetes. In research studies EGCG enhanced insulin activity, protected the pancreatic cells by reducing inflammatory cytokines (e.g. IL-1beta), and reduced IFN-gamma-induced nitric oxide production. It affected genes that inhibit activation of NF- kappaB and reduced the level of messenger RNA for the hepatic gluconeogenic enzymes.*
Alpha Lipoic Acid is a potent antioxidant that acts by multiple mechanisms, both physiologically and pharmacologically, in the treatment of diabetic peripheral neuropathy and hypertension.
In higher doses, alpha lipoic acid supports insulin regulation of blood sugar levels.*
Chromium: The Albion® patented process that combines chromium with glycinate and niacin increases its bioavailability and improves insulin sensitivity. Individuals with Type 2 diabetes tend to have lower blood chromium levels. Chromium enhances the metabolic action of insulin and may reduce some of the risk factors for cardiovascular disease, especially in overweight individuals.*
Directions:
Take two capsules twice daily or as directed by your healthcare practitioner.
References:
Anderson RA, et. al. Isolation and characterization of polyphenol type-A polymers from cinnamon with insulin-like biological activity. J Agric Food Chem. 2004 Jan 14;52(1):65-70. [PMID:14709014]
Imparl-Radosevich J, et.al. Regulation of PTP-1 and insulin receptor kinase by fractions from cinnamon: implications for cinnamon regulation of insulin signaling. Horm Res. 1998 Sep; 50(3):177-82 [PMID: 9762007]
Anderson RA, et al. Isolation and characterization of polyphenol type-A polymers from cinnamon with insulin-like biological activity. J Agric Food Chem. 2004 Jan 14:52(1):65-70. [PMID: 14709014]
Khan A, Safder M, Ali Khan MM, Khattak KN, Anderson RA. Cinnamon improves glucose and lipids of people with type 2 diabetes. Diabetes Care. 2003 Dec; 26(12):3215-8. [PMID: 14633804]
Rotshtyen Y, Zito SW, Application of modified in vitro screening procedure for identifying herbals possessing sulfonylurea-like activity. J Ethnopharmacol. 2004 Aug;93 (2-3):337-44 [PMID: 15234774]
Sievenpiper JL, Arnason JT, Leiter LA, Vuksan V. Variable effects of American Ginseng: a batch of American ginseng (Panax quinquefolius L.) with a depressed ginesenoside profile does not affect postprandial glycemia. Eur J Clin Nutr. 2003 Feb; 57 (2):243-8 [PMID: 12571655]
Shanmugasundaram, E.R.B., et.al. Use of gynema slyvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus. J of Etnopharmacol 1990;30:228-94 [PMID: 2259216]
Rizvi SI, Zaid MA, Anis R, Mishra N. Protective role of tea catechins against oxidation-induced damage of type 2 diabetic erythrocytes. Clin Exp Pharmacol Physiol. 2005 Jan-Feb; 32 (1-2): 70-5 [PMID: 15730438]
Anderso n RA, Polansky MM Tea enchances insulin activity. J Agric Food Chem. 2002 Nov 20; 50(24): 7182-6. [PMID: 12428980]
Koyama Y et.al. Effects of green tea on gene expression of hepatic gluconeogenic enzymes in vivo. Planta Med. 2004 Nov; 70(11):1100-2 [PMID: 15549673]
Han MK. Epigallocatechin gallate, a constituent of green tea, supresses cytokine-induced pancreatic beta-cell damage. Exp Mol Med. 2003 Apr 30;35(2):136-9 [PMID:12754418]
Negrisanu G, Rosu M, Bolte B, Lefter D, Dabelea D Effects of 3-month treatment with the antioxidant alpha-lipoic acid in diabetic peripheral neuropathy. Rom J Intern Med. 1999 Jul-Sep;37(3):297-306 [PMID: 15532308]
de Champlain J. et.al. Oxidative stress in hypertension. Clin Exp Hypertens. 2004 Oct-Nov; 26 (7-8): 593-601 [PMID: 15702613]
Preuss HG, Bagchi M. Protective effects of novel niacin-bound chromium complex and a grape seed proanthocyanidin extract on advancing age and various aspecs of syndrome X. Ann NY Acad Sci. 2002 May; 957:250-9. [PMID: 12074977]
L-carnitine is a conditionally essential micronutrient synthesized from the essential amino acids L-lysine and L-methionine primarily in the human brain, liver, and kidney. Production is a multi-step process and requires adequate niacin, pyridoxine, vitamin C, and iron. Once synthesized, carnitine is transported to other parts of the body, especially cardiac and skeletal muscle where 98% of total body carnitine is confined.*
Carnitine plays an important role in fat and carbohydrate metabolism and energy production by transporting long-chain fatty acids into the mitochondria where beta-oxidation of the fatty acids produces energy in the form of ATP (adenosine-5’-triphosphate). It transports short- and medium-chain fatty acids out of the mitochondria and assists in the liberation of coenzyme A, further promoting ATP synthesis. Carnitine facilitates oxidation of glucose, branched-chain amino acids, and ketones, and is required for the oxidation of medium-chain fatty acids in cardiac and skeletal muscle, tissues that use fatty acids as their primary fuel.*
Carnitine requirements may vary under certain conditions—for example, overnutrition or aging—and supplementation may support energy and glucose metabolism during these times. Researchers studying carnitine function and requirements utilized supplementation to support energy and substrate metabolism in an animal model.
The results suggested that orally administered L-carnitine does indeed support complete fatty acid oxidation, normal mitochondrial fuel metabolism, and glucose tolerance. According to the Council
for Responsible Nutrition, the observed safe level for carnitine supplementation in humans appears to be 2,000 mg per day, although higher doses have been tested and tolerated.*
Muscle fuel metabolism also depends on carnitine when fatty acids become the primary energy source for muscles during ongoing low to moderate exercise. Increasing total muscle carnitine content in healthy humans may support physiological function by reducing muscle glycolysis and increasing glycogen storage, fat oxidation, and work output. A randomized, placebo-controlled human subject study suggested that carnitine can improve exercise tolerance and inspiratory muscle strength, as well as reduce lactate production. A six-month, randomized, double-blind, placebo-controlled study of 50 children suggested that oral supplementation with L-carnitine helped support normal carnitine levels in the body with statistically significant positive effects on support of lung function.*
The role of carnitine in normal fertility has been investigated with meta-analysis of nine randomized controlled trials suggesting that carnitine may be effective in improving pregnancy rate and sperm kinetics, though further research is warranted. In some individuals, carnitine supplementation may support cardiovascular health and triglyceride and HDL levels already within the normal range.*
Carnitine participates in cell volume and fluid balance, liver lipid metabolism, and antioxidant activity. Ongoing research suggests that carnitine supplementation may effectively help maintain the health and function of the cardiovascular, nervous, immune, and endocrine systems, as well as the kidneys and the liver.*
Directions:
Take one capsule twice daily between meals, or as directed by your healthcare practitioner.
References:
Natural Standard Database. www.NaturalStandard.com. Accessed February 24, 2012.
Linus Pauling Institute. http://lpi.oregonstate.edu/infocenter/othernuts/ carnitine/. Accessed February 24, 2012.
Noland RC, Koves TR, Seiler SE, et al. Carnitine insufficiency caused by aging and overnutrition compromises mitochondrial performance and metabolic control. J Biol Chem. 2009 Aug 21;284(34):22840-52. [PMID: 19553674]
Hathcock JN, Shao A. Risk assessment for carnitine. Regul Toxicol Pharmacol. 2006 Oct;46(1):23-8. Review. [PMID: 16901595]
Stephens FB, Constantin-Teodosiu D, Greenhaff PL. New insights concerning the role of carnitine in the regulation of fuel metabolism in skeletal muscle. J Physiol. 2007 Jun 1;581(Pt 2):431-44. Review. [PMID: 17331998]
Wall BT, Stephens FB, Constantin-Teodosiu D, et al. Chronic oral ingestion of L-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. J Physiol. 2011 Feb 15;589(Pt 4):963-73. [PMID: 21224234]
Borghi-Silva A, Baldissera V, Sampaio LM, et al. L-carnitine as an ergogenic aid for patients with chronic obstructive pulmonary disease submitted to whole- body and respiratory muscle training programs. Braz J Med Biol Res. 2006 Apr;39(4):465-74. [PMID: 16612469]
Al-Biltagi M, Isa M, Bediwy AS, et al. L-carnitine improves the asthma control in children with moderate persistent asthma. J Allergy (Cairo). 2012;2012:509730. [PMID: 22162707]
Zhou X, Liu F, Zhai S. Effect of L-carnitine and/or L-acetyl-carnitine in nutrition treatment for male infertility: a systematic review. Asia Pac J Clin Nutr. 2007;16 Suppl 1:383-90. Review. [PMID: 17392136]
Vacha GM, Giorcelli G, Siliprandi N, et al. Favorable effects of L-carnitine treatment on hypertriglyceridemia in hemodialysis patients: decisive role of low levels of high-density lipoprotein-cholesterol. Am J Clin Nutr. 1983 Oct;38(4):532-40. [PMID: 6624695]
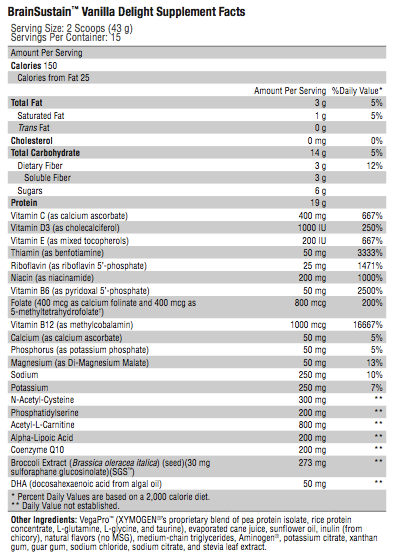
N-Acetyl-Cysteine (NAC) As a source of the conditionally essential amino acid cysteine, NAC is a precursor to one of the brain’s most important antioxidants—glutathione. NAC itself is an effective antioxidant and has been shown to reduce the formation of free radicals that can contribute to oxidative stress in the brain.*
Phosphatidylserine A phospholipid that is highly concentrated in
the brain, phosphatidylserine (PS) plays a key role in neuronal energy production and communication. Since very little PS is found in food, we must synthesize or supplement the amount we need for brain health. For some individuals, decreases in brain function may
be related to “age-related decline in nutrition,” and early nutrition intervention may be warranted. BrainSustain contains safe-source PS from non-GMO soy and contains no animal products.*
Acetyl-L-Carnitine (ALCAR) The ALCAR form of the amino acid L-carnitine is found to have multifaceted roles in supporting nerve health. It is able to cross the blood-brain barrier where it stabilizes cell membranes, acts as an effective antioxidant, and protects brain cells from toxic chemicals and stress-induced damage. In addition, ALCAR supports neuronal energy production, facilitates transport of fuel and waste products into and out of mitochondria, and supports production of acetylcholine, a neurotransmitter essential to the processes of learning and concentration.*
Alpha-Lipoic Acid Acting as both a fat- and water-soluble antioxidant, alpha-lipoic acid provides intracellular and extracellular protection against oxidative stress. With its low molecular weight, alpha-lipoic acid is easily absorbed in the gastrointestinal tract. It then enters circulation, crosses the blood-brain barrier, and reaches the brain where it can regenerate other important antioxidants, including glutathione, vitamin E, and vitamin C.*
Coenzyme Q10 (CoQ10) CoQ10 plays a pivotal role in energy generation because it transports electrons in the mitochondrial electron transport chain. CoQ10 also donates electrons, making it an effective antioxidant that may protect the brain from oxidative stress which is believed to be detrimental to neuronal cells.*
BroccoliSeedExtract The patented form of the phytochemical in broccoli called sulforaphane glucosinolate (SGSTM) is a key ingredient in BrainSustain. Extensive research demonstrates that when SGS is broken down to sulforaphane (its active form), it safely and effectively upregulates the Nrf2 system, enhances antioxidant production, and activates vital phase II detoxification enzymes. This process provides protection from common toxins and xenobiotics.*
DHA(docosahexaenoic acid) A conditionally essential fatty acid, DHA is the main polyunsaturated fatty acid in the brain. DHA supports the structure and function of brain cell membranes, and hence plays a fundamental role in neuronal communication. Studies also indicate that DHA is found to support the biosynthesis and accumulation of PS in neuronal and glial cells.*
VegaPro XYMOGEN’s proprietary pea/rice protein blend VegaPro is coupled with Aminogen® to facilitate protein digestion and absorption, and is lactose free. Amino acids from protein metabolism provide the precursors needed for neurotransmitter production.*
Micronutrients BrainSustain adult formula contains additional micronutrients for neurosupport, including magnesium, calcium, phosphorus, vitamin D3, vitamin E (as mixed tocopherols), and activated B vitamins riboflavin 5’-phosphate (B2), pyridoxal 5’-phosphate (B6), methylcobalamin (B12), and 5-methyltetrahydrofolate (folate). 5-MTHF (5-methyltetrahydrofolate) supports healthy folate nutrition, especially in those with genetic variations in folate metabolism. In BrainSustain, 5-MTHF is provided as Quatrefolic® for enhanced stability, solubility, and bioavailability.[18] In addition, two scoops of BrainSustain adult formula provide the same amount of NAC, PS, ALCAR, alpha-lipoic acid, CoQ10, and SGS as eight capsules of NeuroActivesTM BrainSustainTM.*
Directions:
Blend, shake, or briskly stir two level scoops (43 g) of BrainSustainTM into 8-12 oz chilled water, or as directed by your healthcare practitioner. Adjust amount of water to desired sweetness and/or thickness.
Directions:
For children four years of age or older, blend, shake, or briskly stir 1 level scoop (20 grams) of BrainSustain for KidsTM into 4-6 oz chilled water or other beverage, or as directed by your healthcare practitioner. Adjust amount of water to desired sweetness and/or thickness.
References:
Sansone RA, Sansone LA. Getting a knack for NAC: N-acetyl-cysteine. Innov Clin Neurosci. 2011 Jan;8(1):10-4. [PMID: 21311702]
Kato-Kataoka A, Sakai M, Ebina R, et al. Soybean-derived phosphatidylserine improves memory function of the elderly Japanese subjects with memory complaints. J Clin Biochem Nutr. 2010 Nov;47(3):246-55. [PMID: 21103034]
Richter Y, Herzog Y, Cohen T, et al. The effect of phosphatidylserine-containing omega-3 fatty acids on memory abilities in subjects with subjective memory complaints: a pilot study. Clin Interv Aging. 2010 Nov 2;5:313-6. [PMID: 21103402]
Vakhapova V, Cohen T, Richter Y, et al. Phosphatidylserine containing omega-3 fatty acids may improve memory abilities in non-demented elderly with memory complaints: a double-blind placebo-controlled trial. Dement Geriatr Cogn Disord. 2010;29(5):467- 74. [PMID: 20523044]
Suchy J, Chan A, Shea TB. Dietary supplementation with a combination of alpha- lipoic acid, acetyl-L-carnitine, glycerophosphocoline, docosahexaenoic acid, and phosphatidylserine reduces oxidative damage to murine brain and improves cognitive performance. Nutr Res. 2009 Jan;29(1):70-4. [PMID: 19185780]
Picconi B, Barone I, Pisani A, et al. Acetyl-L-carnitine protects striatal neurons against in vitro ischemia: the role of endogenous acetylcholine. Neuropharmacology. 2006 Jun;50(8):917-23. [PMID: 16500685]
Steffen V, Santiago M, de la Cruz CP, et al. Effect of intraventricular injection of 1-methyl-4-phenylpyridinium: protection by acetyl-L-carnitine. Hum Exp Toxicol. 1995 Nov;14(11):865-71. [PMID: 8588946]
Sorbi S, Forleo P, Fani C, et al. Double-blind, crossover, placebo-controlled clinical trial with L-acetylcarnitine in patients with degenerative cerebellar ataxia. Clin Neuropharmacol. 2000 Mar-Apr;23(2):114-8. [PMID: 10803803]
Jones LL, McDonald DA, Borum PR. Acylcarnitines: role in brain. Prog Lipid Res. 2010 Jan;49(1):61-75. Review. [PMID: 19720082]
Kobayashi S, Iwamoto M, Kon K, et al. Acetyl-L-carnitine improves aged brain function. Geriatr Gerontol Int. 2010 Jul;10 Suppl 1:S99-106. [PMID: 20590847]
Packer L, Tritschler HJ, Wessel K. Neuroprotection by the metabolic antioxidant alpha- lipoic acid. Free Radic Biol Med. 1997;22(1-2):359-78. Review. [PMID: 8958163]
Liu J. The effects and mechanisms of mitochondrial nutrient alpha-lipoic acid on improving age-associated mitochondrial and cognitive dysfunction: an overview. Neurochem Res. 2008 Jan;33(1):194-203. Review. [PMID: 17605107]
Mancuso M, Orsucci D, Volpi L, et al. Coenzyme Q10 in neuromuscular and neurodegenerative disorders. Curr Drug Targets. 2010 Jan;11(1):111-21. Review. [PMID: 20017723]
Ping Z, Liu W, Kang Z, et al. Sulforaphane protects brains against hypoxic-ischemic injury through induction of Nrf2-dependent phase 2 enzyme. Brain Res. 2010 Jul 9;1343:178-85. [PMID: 20417626]
Vauzour D, Buonfiglio M, Corona G, et al. Sulforaphane protects cortical neurons against 5-S-cysteinyl-dopamine-induced toxicity through the activation of ERK1/2, Nrf-2 and the upregulation of detoxification enzymes. Mol Nutr Food Res. 2010 Apr;54(4):532-42. [PMID: 20166144]
Chang CY, Ke DS, Chen JY. Essential fatty acids and human brain. Acta Neurol Taiwan. 2009 Dec;18(4):231-41. Review. [PMID: 20329590]
Guo M, Stockert L, Akbar M, et al. Neuronal specific increase of phosphatidylserine by docosahexaenoic acid. J Mol Neurosci. 2007 Sep;33(1):67-73. [PMID: 17901548]
Quatrefolic®. http://quatrefolic.com. Accessed September 26, 2011.
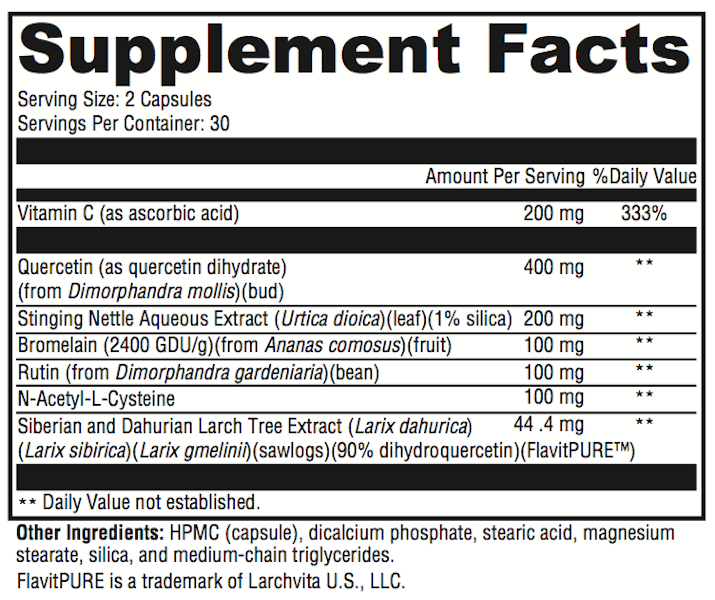
Individuals with hypersensitive immune reactions often experience physical, mental, and functional decline even with moderate onset of discomfort.[1] AllerDHQ provides fast-acting, natural support for hypersensitivity reactions, including watery, itchy eyes and runny nose, as well as other manifestations of histamine release. Formulated with a synergistic combination of vitamins, bioflavonoids, amino acids, herbs, and bromelain, AllerDHQ addresses the distressing signs of immune hypersensitivity.*
Vitamin C (ascorbic acid) Vitamin C is essential to humans and must be obtained exogenously. While most mammals are able to synthesize ascorbic acid, humans lack one of the enzymes required for this process and can quickly become deficient if dietary or supplemental intake is inadequate. Stress, smoking, pollution, and temperature changes increase our requirement for vitamin C. Well-known functions of vitamin C include antioxidant protection from damaging free radicals and the synthesis of collagen, carnitine, and neurotransmitters. Vitamin C also plays a lesser-known role in the deactivation of histamine.*
Bioflavonoids Quercetin, dihydroquercetin (DHQ), and rutin are active bioflavonoids incorporated into Allergy Revolution for their role in moderating an exaggerated immune response. Bioflavonoids work synergistically with other antioxidants to protect tissues from the negative effects of oxidation and inflammation often observed during hyperimmune reactions. Immune-moderating effects include inhibition of mast-cell degranulation and prevention of histamine release during hypersensitive episodes.*
Dihydroquercetin DHQ supports the activities of other antioxidants, protects erythrocytes and capillaries, supports bronchial function, and assists in chelation of metals. DHQ was also found to moderate pro-inflammatory pathways by inhibiting inducible ICAM-1 expression. The FlavitPURETM† form of DHQ in Allergy Revolution is a bioactive, natural form that is significantly more absorbable than quercetin alone. The inclusion of FlavitPURE in Allergy Revolution creates a clear advantage over products containing only quercetin, as fewer capsules are required for effective results. This specific form of DHQ boasts an impressive ORAChydro value of 28,000+ μM TE/g and a CAP-e assay of 9.9-10.5 units per gram, indicative of effective antioxidant protection within the cell. ORAChydro reflects oxygen radical absorbance capacity for water-soluble antioxidants, and CAP-e refers to cell- based antioxidant protection in erythrocytes.*
Rutin A source of naturally occurring flavonoids, rutin reduces capillary permeability and edema, which can reduce mucus fluid buildup or “runny nose.”[10] Rutin’s protective effect against oxidation is amplified by ascorbic acid, also present in Allergy Revolution.*
N-Acetyl-Cysteine NAC is the acetylated form of the conditionally essential amino acid L-cysteine. As a precursor to the “master antioxidant” glutathione, NAC plays a significant role in detoxification and antioxidant protection. NAC also functions as a natural mucolytic, reducing the viscosity of mucus commonly produced during a hyperimmune response.*
Stinging Nettle Extract (Urtica dioica) Stinging nettle leaf has been found to regulate a variety of inflammatory activities associated with hyperimmune response, including mast-cell degranulation, prostaglandin formation, and histamine action.*
Bromelain Bromelain refers to an enzyme complex extracted from the stem and fruit of the pineapple plant (Ananas comosus). Its modulation of the inflammatory response is thought to exert a beneficial effect in combating hypersensitive immune reactions, earning it approved status by the German Commission E for “micro-inflammations” and related discomforts. Early studies identified its positive effects on controlling edema, tissue permeability, and vasodilation. Bromelain is also found to enhance the absorption of quercetin.*
Research indicates that the natural components in AllerDHQ, including vitamin C, bioflavonoids, DHQ, NAC, and bromelain, work synergistically to moderate unpleasant immune reactions.*
Directions:
Take one to two capsules daily, or as directed by your healthcare practitioner.
Children and individuals using blood thinners should consult their healthcare practitioner prior to use. Do not use if tamper seal is damaged.
References:
1. Thornhill SM, Kelly AM. Natural treatment of perennial allergic rhinitis. Altern Med Rev. 2000 Oct;5(5):448-54. [PMID: 11056414]
2. Johnston CS. The antihistamine action of ascorbic acid. Subcell Biochem. 1996;25:189-213. [PMID: 8821975]
3. Strohle A, Wolters M, Hahn A. Micronutrients at the interface between inflammation and infection—ascorbic acid and calciferol: part 1, general overview with a focus on ascorbic acid. Inflamm Allergy Drug Targets. 2011 Feb;10(1):54-63. [PMID: 21184650]
4. Skaper SD, Fabris M, Ferrari V, et al. Quercetin protects cutaneous tissue-associated cell types including sensory neurons from oxidative stress induced by glutathione depletion: cooperative effects of ascorbic acid. Free Radic Biol Med. 1997;22(4):669-78. [PMID: 9013129]
5. Middleton E Jr, Drzewiecki G, Krishnarao D. Quercetin: an inhibitor of antigen-induced human basophil histamine release. J Immunol. 1981 Aug;127(2):546-50. [PMID: 6166675]
6. Park HH, Lee S, Son HY, et al. Flavonoids inhibit histamine release and expression of proinflammatory cytokines in mast cells. Arch Pharm Res. 2008 Oct;31(10):1303-11. [PMID: 18958421]
7. http://www.vitalavita.us Accessed July 31, 2011.
8. Bito T, Roy S, Sen CK, et al. Flavonoids differentially regulate IFN gamma-induced ICAM-1 expression in human keratinocytes: molecular mechanisms of action. FEBS Lett. 2002 Jun 5;520(1-3):145-52. [PMID: 12044887]
9. Ou B, Hampsch-Woodill M, Prior RL. Development and validation of an improved oxygen radical absorbance capacity assay using fluorescein as the fluorescent probe. J Agric Food Chem. 2001 Oct;49(10):4619-26. [PMID: 11599998]
10. Turner RB, Fowler SL, Berg K. Treatment of the common cold with troxerutin. APMIS. 2004 Sep;112(9):605-11. [PMID: 15601310]
11. Kelly GS. Clinical applications of N-acetylcysteine. Altern Med Rev. 1998 Apr;3(2):114-27. [PMID: 9577247]
12. Ziment I. Acetylcysteine: a drug that is much more than a mucokinetic. Biomed Pharmacother. 1988;42(8):513-9. [PMID: 3066412]
13. Roschek B Jr, Fink RC, McMichael M, Alberte RS. Nettle extract (Urtica dioica) affects key receptors and enzymes associated with allergic rhinitis. Phytother Res. 2009 Jul;23(7):920-6. [PMID: 19140159]
14. Riehemann K, Behnke B, Schulze-Osthoff K. Plant extracts from stinging nettle (Urtica dioica), an antirheumatic remedy, inhibit the proinflammatory transcription factor NF-kappaB. FEBS Lett. 1999 Jan 8;442(1):89-94. [PMID: 9923611]
15. Blumenthal M. The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines. Austin, TX: American Botanical Council; 2000.
16. Maurer HR. Bromelain: biochemistry, pharmacology and medical use. Cell Mol Life Sci. 2001 Aug;58(9):1234-45. [PMID: 11577981]
17. Ryan RE. A double-blind clinical evaluation of bromelains in the treatment of acute sinusitis. Headache. 1967 Apr;7(1):13-7. [PMID: 4859824]
18. Lakhanpal, P, Rai DK. Quercetin: A Versatile Flavonoid. IJMU. 2007 Jul-Dec;2(2):22-37.
Alpha-lipoic acid (ALA) is an eight-carbon disulfide water- and fat- soluble compound that is synthesized in small quantities in the liver and other tissues. Oral supplementation readily crosses the blood brain barrier after it is absorbed in the small intestine, goes into the portal vein, and is distributed via systemic circulation. Once in the tissues, ALA can be found inside and outside the cells including inside the mitochondria where it functions naturally as a coenzyme for the oxidation of pyruvate, alpha ketoglutarate, and branched-chain amino acids.*
Researchers recently identified lipoic acid’s mechanisms of action related to maintaining metabolic health. It has a direct binding site at the insulin receptor tyrosine kinase domain. ALA appears to modulate 5’-AMP-activated protein kinase and PPAR-regulated genes, to activate PPAR–alpha and PPAR-gamma, and to support expression of PPAR-gamma mRNA and protein in heart tissue and smooth muscle of the aorta.*
Controlled-release technology supports efficacy of alpha-lipoic acid in helping to maintain blood sugar already in the normal range.
Data from a 12-week clinical study indicate that supplementation with ALAmax CR TM (1200 mg per day, divided doses) may support healthy C-peptide levels. C-peptide is used as an indication of insulin sensitivity.*
Alpha-lipoic acid effectively neutralizes a variety of free radicals, including oxygen radicals and ionized metals. This action is particularly beneficial for people who have higher levels of oxidative stress. Alpha- lipoic acid regenerates vitamins C and E, increases tissue levels of glutathione, and helps maintain the proper ratio of reduced to oxidized coenzyme Q10 in the mitochondria. In addition, alpha-lipoic acid may help the body rid itself of heavy metals.*
Healthy endothelial-mediated vasodilation is accepted as a surrogate marker for cardiovascular health and can be affected by synthesis, bioavailability, or action of nitric oxide (NO). Increased oxidative stress appears to play a significant role in neutralizing or inactivating NO. ALA’s antioxidant properties, along with its demonstrated safety and potency, qualify it as a prime candidate to evaluate for its ability to support healthy endothelial function.*
The ability of alpha-lipoic acid to improve energy metabolism and decrease oxidative stress alludes to its ability to support healthy mitochondrial function with age.*
Biotin has been added because chronic administration of lipoic acid lowers the activities of pyruvate carboxylase and beta-methylcrotonyl- CoA carboxylase in vivo by competing with biotin.*
Directions:
Take 1 tablet 30 minutes before breakfast and 1 tablet 30 minutes before dinner, or as directed by your healthcare practitioner.
References:
Teichert J, Kern J, Tritschler HJ, Ulrich H, Preiss R: Investigations on the pharmacokinetics of alpha-lipoic acid in healthy volunteers. Int.J.Clin. Pharmacol.Ther. 36:625-628, 1998
Pershadsingh HA. Alpha-lipoic acid: physiologic mechanisms and indications for the treatment of metabolic syndrome. Expert Opin Investig Drugs. 2007 Mar;16(3):291-302 [PMID: 17302524]
Evans JL, Goldfine ID: α-Lipoic acid: a multi-functional antioxidant that improves insulin sensitivity in patients with type 2 diabetes. Diabetes Technol Therap 2:401-413, 2000
Jacob S, Ruus P, et al. Oral administration of RAC-alpha-lipoic acid modulates insulin sensitivity in patients with type 2 diabetes mellitus: a placebo-controlled pilot trial. Free Radic Biol Med 27:309-314, 1999
Bojunga J, et al. Antioxidative treatment reverses imbalances of nitric oxide synthase isoform expression and attenuates tissue-cGMP activation in diabetic rats. Biochem Biophys Res Commun. 2004 Apr 9;316(3):771-80 [PMID: 15033467]
Zempleni J, Trusty TA, Mock DM. Lipoic acid reduces the activities of biotin- dependent carboxylases in rat liver. J Nutr. 1997 Sep;127(9):1776-81 [PMID: 9278559]
Foster TS. Efficacy and safety of {alpha}-lipoic acid supplementation in the treatment of symptomatic diabetic neuropathy. Diabetes Educ. 2007 Jan- Feb;33(1):111-7 [PMID: 17272797]
Diesel B. et. al. Alpha-lipoic acid as a directly binding activator of the insulin receptor: protection from hepatocyte apoptosis. Biochemistry. 2007 Feb 27;46(8):2146-2155. Epub 2007 Feb 3 [PMID: 17274632]
LipiChol, also known as Onemia, is a patented medical food formulated for the clinical dietary management of omega-3 phospholipid deficiency, a condition which can lead to an increase in cardiovascular risk factors and unfavorable metabolic changes.As a medical food, LipiChol is to be used under the supervision of a licensed health care practitioner and requires a prescription.
Omega-3 Fatty Acids Healthy omega-3 phospholipid status affects cell membrane function and cardiometabolic health. EPA and DHA have been extensively studied for their positive effects on cardiovascular health, cognitive integrity, immune function, and the natural response to inflammation.[1,2] Research suggests that serum EPA and DHA, which reflect dietary intake, are inversely associated with mortality, cardiovascular risk, and sudden cardiac death.[3,4] The omega-3 index, a measurement of erythrocyte EPA plus DHA, has become recognized as a biomarker of cardiovascular health.[4] Clinical trials suggest that LipiChol promotes an improvement in omega-3 index.[5]
Adequate serum and cell-membrane levels of EPA/DHA are crucial to cell function. Many individuals have a limited ability to convert the parent omega-3 alpha-linolenic acid (ALA) to EPA and DHA; therefore, adequate intake of preformed EPA and DHA is necessary.[6] This is why we generally do not recommend taking Flax Seed Oil as a source of Omega-3’s as it is simply ALA and doesn’t produce the needed results.
LipiChol provides EPA and DHA in a concentrated, bioavailable, phospholipid form found to positively affect blood lipids, including triglycerides, to a greater extent than the triglyceride or ethyl-ester form of fish oil does. [5,6] Some studies suggest that fish oil may increase low density lipoprotein (LDL) levels,[1,7,8] while krill oil may decrease LDL.[9]
Phospholipids Considered the building blocks of healthy cells, phospholipids are water- and fat-soluble and help maintain cell membrane fluidity and function. The phospholipid form (versus triglyceride form) of omega-3 EPA and DHA is easily recognized, integrated, and utilized by the body’s cells.
Healthy phospholipid levels are important to maintaining normal levels of high density lipoprotein (HDL), serum triglycerides, and cardiovascular health as well. Phosphatidylcholine (PC)—the major phospholipid found in LipiChol—is highly concentrated in the brain, heart, liver, and kidneys.[10] PC is a source of choline for acetylcholine production and may directly support cardiovascular health by participating in the metabolism of homocysteine.[11,12] RevChol’s marine phospholipids are a concentrated 53-58% purified phospholipid (PPL), 80% of which occurs as phosphatidylcholine.
Antarctic Krill (Euphausia superba) Krill, a coldwater marine crustacean, is a rich source of omega-3 EPA and DHA. Krill oil has been used in several human clinical trials, and research consistently suggests that krill omega-3 phospholipids support antioxidant activity, healthy cell membranes, healthy blood lipids, and the normal response to inflammation.[13-15] Krill is low on the food chain and is considered a sustainable source of nutrients. Precautionary catch limits are established by the Commission for the Conservation of Antarctic Marine Living Resources (CCAMLR).[16]
Astaxanthin As a red-orange member of the carotenoid family, astaxanthin provides antioxidant activity. Both animal and clinical research suggest that astaxanthin supports antioxidant mechanisms as well as a healthy response to inflammation.[17] Krill is recognized as a rich source of astaxanthin and a potentially valuable contributor to cardiovascular health.[14]
Research The chemical form of omega-3 fatty acids can determine their bioavailability. A double-blind crossover trial compared uptake of EPA/DHA from krill (mainly phospholipid form) to uptake from two forms of fish oil—re-esterified triacylglycerides (rTAG) and ethyl- esters (EE). Results suggested that krill oil had superior bioavailability and promoted the highest incorporation of EPA and DHA into plasma phospholipids.[18] A multi-center, three-month, prospective, randomized, double-blind, placebo-controlled study compared the effects of krill oil versus fish oil on serum lipids. Results suggested krill oil reduced total cholesterol, LDL, and triglycerides, while it increased HDL, improving each of these parameters to a greater extent than 3 g of fish oil did. Results were even more dramatic with higher doses of krill oil. Doses of 1-1.5 g krill oil per day appeared to support healthy blood glucose metabolism as well.[9]
A randomized double-blind parallel arm trial of 76 subjects indicated that 2 g krill oil per day significantly increased plasma EPA and DHA levels and was well tolerated.[19] Highly concentrated krill oil, LipiChol’s main component, was administered to a total of 203 subjects in six clinical trials with no serious side effects observed at a dose up to 6g/day.[12] This concentrated form of krill oil was found to decrease serum triglycerides to levels similar to prescribed fish oil found in the market place.[5] Clinical trials also noted a better and faster improvement of the omega-3 index using concentrated krill oil in comparison to fish oil.[5]
Directions
Take 2 capsules daily – be sure to take them with the largest meal of the day. Taking them with the largest meal of the day seems to impact the absorption and the clinic results as well. If we do not see the benefits we are seeking then we may increase the dose to 3 capsules daily.
References
Linus Pauling Institute. http://lpi.oregonstate.edu/infocenter/othernuts/ omega3fa/#metabolism. Accessed April 20, 2012.
GOED. http://www.goedomega3.com/clinical-studies.html. Accessed April 20, 2012.
Pottala JV, Garg S, Cohen BE, et al. Blood eicosapentaenoic and docosahexaenoic acids predict all-cause mortality in patients with stable coronary heart disease: the Heart and Soul study. Circ Cardiovasc Qual Outcomes. 2010 Jul;3(4):406-12. [PMID: 20551373]
Harris WS. The omega-3 index as a risk factor for coronary heart disease. Am J Clin Nutr. 2008 Jun;87(6):1997S-2002S. [PMID: 18541601]
Onemia. http://onemia.com/professional/studies.php. Accessed May 8, 2012.
Gerster H. Can adults adequately convert alpha-linolenic acid (18:3n-3) to eicosapentaenoic acid (20:5n-3) and docosahexaenoic acid (22:6n-3)? Int J Vitam Nutr Res. 1998;68(3):159-73. Review. [PMID: 9637947]
Hartweg J, Perera R, Montori V,et al. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD003205. [PMID: 18254017]
Montori VM, Farmer A, Wollan PC, et al. Fish oil supplementation in type 2 diabetes: a quantitative systematic review. Diabetes Care. 2000 Sep;23(9):1407-15. [PMID: 10977042]
Bunea R, El Farrah K, Deutsch L. Evaluation of the effects of Neptune Krill Oil on the clinical course of hyperlipidemia. Altern Med Rev. 2004 Dec;9(4):420-8. [PMID: 15656713]
Phosphatidylcholine. Natural Standard Database. http://naturalstandard.com/ databases/herbssupplements/phosphatidylcholine.asp. Accessed April 16, 2012.
Olthof MR, Brink EJ, Katan MB, et al. Choline supplemented as phosphatidylcholine decreases fasting and postmethionine-loading plasma homocysteine concentrations in healthy men. Am J Clin Nutr. 2005 Jul;82(1):111-7. [PMID: 16002808]
Onemia. http://onemia.com/professional/professional.php. Accessed April 16, 2012.
Tou JC, Jaczynski J, Chen YC. Krill for human consumption: nutritional value and potential health benefits. Nutr Rev. 2007 Feb;65(2):63-77. Review. [PMID: 17345959]
Deutsch L. Evaluation of the effect of Neptune Krill Oil on chronic inflammation and arthritic symptoms. J Am Coll Nutr. 2007 Feb;26(1):39-48. [PMID: 17353582]
CCAMLR. http://www.ccamlr.org/pu/E/sc/kri-surv-intro.htm. Accessed April 16, 2012
Hussein G, Sankawa U, Goto et al. Astaxanthin, a carotenoid with potential in human health and nutrition. J Nat Prod. 2006 Mar;69(3):443-9. Review. [PMID: 16562856]
Schuchardt JP, Schneider I, Meyer H, et al. Incorporation of EPA and DHA into plasma phospholipids in response to different omega-3 fatty acid formulations—a comparative bioavailability study of fish oil vs. krill oil. Lipids Health Dis. 2011 Aug 22;10:145. [PMID: 21854650]
Maki KC, Reeves MS, Farmer M, et al. Krill oil supplementation increases plasma concentrations of eicosapentaenoic and docosahexaenoic acids in overweight and obese men and women. Nutr Res. 2009 Sep;29(9):609-15. [PMID: 19854375]
At the same time as the media increases consumer awareness of the importance of fish oils, manufacturers face the challenge of eliminating heavy metals and polychlorinated biphenyls (PCBs). The industry-leading technologies used in the preparation of the fish oils surpass the standards for environmental pollutants, including dioxins, PCBs, pesticides, and heavy metals such as mercury.
OmegaPure oils are processed through special molecular distillation. Molecular distillation is commonly used to purify and concentrate fish oils. In this process, the fish oil is broken down into its basic molecular components and separated by molecular weight. Due to varying molecular weights, specific components can be removed from or concentrated in the oil. This ensures that contaminants can be reduced to levels far below industry standards. It also allows the manufacturer to increase the concentration of active ingredients. For example, an 18:12 oil can be concentrated through molecular distillation to produce a 30:20 product, as in the case of OmegaPure 600.
Processing a fish oil formula begins with rigorous care and control of the starting raw materials (non-GMO sardines, mackerel, anchovies) to assure optimum oil quality. The oils are distilled in a controlled, pristine vacuum environment to minimize distillation temperatures. The exposure time, even to these lower distillation temperatures, is tightly controlled and uniform, resulting in levels of impurities well below the industry standards. The technology employed for OmegaPure 600 meets special molecular distillation standards. As this oil is a concentrated source of omega-3 fatty acids, our manufacturer goes above and beyond the traditional purification methods to ensure its safety. This is accomplished by:
» A triple-phase molecular distillation purification process to maximize purity while concentrating the EPA and DHA polyunsaturated fatty acids
» Ensuring consistency in contaminant removal, and therefore purity levels, through uniform processing times » Reducing the evaporation stage to half the time of traditional systems to drive down the oxidative risk
The proprietary technologies used in the manufacture of OmegaPure oils are in accordance with pharmaceutical standards that assure safe, consistent fish oils. Furthermore, Revolution Health & Wellness requires regular third-party testing to verify that OmegaPure oils meet the stringent standards we use for freshness, quality, and purity.[1]
Despite aggressive marketing claims to the contrary, a recent publication by Oelrich et al reported that, of the three formulations tested, there was no significant difference in the effect on triglycerides.[2] The active therapy of the three fish oil supplementation arms was 4 g/day of combined EPA and DHA provided as: a) 90% triglyceride (TG) formulation (TG90), b) 60% TG formulation (TG60), or c) ethyl esters (EE) (i.e., 0% TG). Furthermore, omega-3 fish oils provided in an ethyl ester formulation tended to have a lower impact on increasing LDL-cholesterol levels compared to omega-3 fish oils delivered in the triglyceride formulation.*
Research suggests it takes 2 g/day of DHA supplementation for a month to saturate the plasma and three to six months of supplementation to saturate the tissues.[3] Concentrations increase in breast milk within less than a week of DHA supplementation. [3]
Research and studies provide evidence that omega-3 fatty acids antagonize arachidonic acid-induced proinflammatory prostaglandin formation, provide resolvins and protectins to aid the body’s “cleanup” response to the inflammatory cascade, promote neurological health and mental functioning, support a balanced immune response, and support healthy glucose and insulin metabolism.[4-13] Furthermore, supportive but not conclusive research shows that consumption of EPA and DHA omega-3 fatty acids may reduce the risk of coronary heart disease.*[13-16]
Directions
Take 1-2 capsules one to three times daily. We generally guide the dosing recommendations based on lab evaluation of your Omega-3 Index.
References
Assays available upon request.
Oelrich B, Dewell A, Gardner CD. Effect of fish oil supplementation on serum triglycerides, LDL cholesterol and LDL subfractions in hypertriglyceridemic adults. Nutr Metab Cardiovasc Dis. 2011 Sep 15. Epub ahead of print. [PMID: 21924882]
Arterburn LM, Hall EB, Oken H. Distribution, interconversion, and dose response of n-3 fatty acids in humans. Am J Clin Nutr. 2006 Jun;83(6 Suppl):1467S- 1476S. Review. [PMID: 16841856]
Storey A, McArdle F, Friedmann PS, et al. Eicosapentaenoic acid and docosahexaenoic acid reduce UVB- and TNF alpha-induced IL-8 secretion in keratinocytes and UVB-induced IL-8 in fibrolasts. J Invest Dermatol. 2005 Jan;124(1):248-55. [PMID: 15654981]
Kim YJ, Kim HJ, No JK, et al. Anti-inflammatory action of dietary fish oil and calorie restriction. Life Sci. 2006 Apr 18;78(21): 2523-32. [PMID: 16438990]
Maroon JC, Bost JW. Omega-3 fatty acids (fish oil) as an anti-inflammatory: an alternative to nonsteroidal anti-inflammatory drugs for discogenic pain. Surg Neurol. 2006 Apr;65(4):326-31. [PMID: 16531187]
Weylandt KH, Chiu CY, Gomolka B, et al. Omega-3 fatty acids and their lipid mediators: Towards an understanding of resolvin and protectin formation. Prostaglandins Other Lipid Mediat. 2012 Mar;97(3-4):73-82. [PMID: 22326554]
Kremmyda LS, Tvrzicka E, Stankova B, et al. Fatty acids as biocompounds: their role in human metabolism, health and disease: a review. part 2: fatty acid physiological roles and applications in human health and disease. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2011 Sep;155(3):195-218. doi: 10.5507/bp.2011.052. [PMID: 22286806]
Frangou S, Lewis M, McCrone P. Efficacy of ethyl-eicosapentaenoic acid in bipolar depression: randomized double-blind placebo-controlled study. Br J Psychiatry. 2006 Jan;188:46-50. [PMID: 16388069]
Kankaanpaa P, Sutas Y, Salminen S, et al. Dietary fatty acids and allergy. Ann Med. 1999 Aug;31(4):282-87. [PMID: 10480759]
Ebbesson SO, Risica PM, Ebbesson LO, et al. Omega-3 fatty acids improve glucose tolerance and components of the metabolic syndrome in Alaskan Eskimos: the Alaska Siberia project. Int J Circumpolar Health. 2005 Sep:64(4):396-408. [PMID:16277123]
Nettleton JA, Katz R. n-3 long-chain polyunsaturated fatty acids in type 2 diabetes: a review. J Am Diet Assoc. 2005 Mar;105(3):428-40. [PMID:15746832]
Weitz D, Weintraub H, Fisher E, et al. Fish oil for the treatment of cardiovascular disease. Cardiol Rev. 2010 Sep-Oct;18(5):258-63. [PMID: 20699674]
Psota TL, Gebauer SK, Kris-Etherton P. Dietary omega-3 fatty acid intake and cardiovascular risk. Am J Cardiol. 2006 Aug 21;98(4A):3i-18i. [PMID: 16919512]
Sasaki J, Yokoyama M, Matsuzaki M, et al. Relationship between coronary artery disease and non-HDL-C, and effect of highly purified EPA on the risk of coronary artery disease in hypercholesterolemic patients treated with statins: sub-analysis of the Japan EPA Lipid Intervention Study (JELIS). J Atheroscler Thromb. 2012;19(2):194-204. [PMID: 22186099]
Zhang J, Wang C, Li L, et al. Inclusion of Atlantic salmon in the Chinese diet reduces cardiovascular disease risk markers in dyslipidemic adult men. Nutr Res. 2010 Jul;30(7):447-54. [PMID: 20797476]
Revolution Health & Wellness Clinic seeks to optimize the health of all patients starting with the foundation of what we call the ‘Healthy Trinity. This consists of 3 components: Nutrition, Exercise, and The 3R’s (Rest, Reduce Stress, and Recovery from Exercise). We then seek to identify problems that require medical intervention and address them accordingly.
We have found that nutrition in addition to ‘drugless prescriptions’ using natural supplements is key to improving health without the numerous side effects and ‘unintended consequences’ associated with most medications.
We only use the highest grade supplements available. All of our supplements are pharmaceutical grade. If it is important to your health then it is important to us!
One of the problems associated with supplements is the poor and inconsistent quality. Supplements are not FDA controlled and, therefore, anyone can produce anything they want. There is no requirement for the label to be consistent with what is actually in the body. This means that there is a significant amount of inconsistency in most supplements.
Quality Matters!
We go to great lengths to ensure that our supplements exceed the standard. Quality truly does matter! Every lot of each of our supplements is independently, 3rd party tested. This means that we send a sample to a testing facility to ensure that it actually has the highest quality and consistency. We have even gone so far as to test our testers! We send samples that are known to not meet the standard to ensure that these samples are appropriately being tested.
Our manufacturing facility, in Orlando, FL, has been certified by the FDA and we have recently been awarded certification by the NSF.
Quite simply, our supplements offer the highest quality, purity, and consistency so that you can be assured that you get nothing but the best at Revolution Health & Wellness!
We are constantly working to expand our line of supplements to better serve the needs of our patients.