PREDIMED Study – Traditional Mediterranean Diet (TMD)
The PREDIMED Study evaluated the Traditional Mediterranean Diet (TMD) for the prevention of Cardiovascular Disease. The Traditional Mediterranean Diet has been a favorite for health advocates for years. Multiple observational and secondary prevention trials showed improvement in risk for Cardiovascular Disease so the authors of the PREDIMED Study conducted a randomized trial to confirm (or debunk) these observations.
The PREDIMED Study was conducted in multiple locations (centers) in Spain. The participants were considered to be at ‘High cardiovascular disease risk’ but had no cardiovascular disease at enrollment. High risk of cardiovascular disease meant that participants were either Type 2 diabetic or at least 3 of the following: smoking, hypertension, elevated LDL, low HDL, overweight/obese, or family history of premature cardiovascular disease.
Mediterranean diet supplemented with mixed nuts (walnuts, almonds, and hazelnuts)
Control diet – they were advised to reduce dietary fat
All participants received educational sessions (individual and group) every quarter. Depending on the group, they were given free extra-virgin olive oil (~1 liter per week), mixed nuts (30 grams per day), or small nonfood gifts. They did not control or adjust caloric intake and there was no promotion of exercise or physical activity.
Mediterranean Diet
Recommended Foods
Olive Oil: >4 tablespoons per day. The amount of olive oil includes oil used for cooking and salads and oil consumed in meals eaten outside the home. In the Mediterranean Diet Olive Oil group, the goal was to consume 50 grams (approximately 4 tablespoons) or more per day of the polyphenol-rich olive oil supplied to them as opposed to the ordinary refined variety, which is low in polyphenols.
Tree nuts and peanuts: > 3 servings per week
Fresh fruits: > 3 servings per day
Vegetables: > 2 servings per day
Fish (especially fatty fish) & Seafood: > 3 servings per week
Legumes: > 3 servings per week
Sofrito: > 2 servings per week. Sofrito is a sauce made with tomato and onion, often including garlic and aromatic herbs, and slowly simmered with olive oil.
White meat: instead of red meat
Wine with meals (optional, only for those already drinking alcohol): > 7 glasses per week
Discouraged Foods
Sodas (soft drinks): < 1 per day
Commercial baked good, sweets, & pastries: <3 servings per day
Spread fats: <1 serving per day
Red and processed meats: < 1 serving per day
Control Diet (low fat)
Recommended Foods
Low-fat dairy products: > 3 servings per day
Bread, potatoes, pasta, rice: > 3 servings per day
Fresh fruits: > 3 servings per day
Vegetables: > 2 servings per day
Lean fish & seafood: > 3 servings per week
Discouraged Foods
Vegetable oils (including olive oil): < 2 tablespoons per day
Fatty fish, seafood canned in oil: < 1 serving per week
Sofrito: < 2 servings per week
Compliance
Compliance with all of the diet groups was good. Biomarkers (hydroxytyrosol for olive oil group & ALA level for mixed nuts group) were measured to confirm compliance.
Participants were followed for 4.8 years. 209 participants (2.8%) opted to not attend subsequent visits. Dropouts were higher in the Control Diet (11.3%) than in the Mediterranean Diet (4.9%).
Increased benefit was noted in the group with dyslipidemia and hypertension in regards to the primary end-point.
Conclusions:
The primary end points (for what they were looking to see if the diet helped) were major cardiovascular disease events (myocardial infarction, stroke, or death from cardiovascular disease causes). The study was conducted for 4.8 years. The study was funded by the Spanish Government (Instituto de Salud Carlos III and others).
There were a total of 7447 participants, 55-80 years of age. The primary end-point (myocardial infarction, stroke, or death from cardiovascular disease causes) occurred in a total of 288 of the participants.
Mediterranean diet with extra-virgin olive oil – 96 events, 30% reduced risk (hazard ratio 0.70)
Mediterranean diet with mixed nuts – 83 events, 28% reduced risk (hazard ratio 0.72)
Control diet – 109 events
The author’s conclusion: “In this study involving persons at high cardiovascular risk, the incidence of major cardiovascular events was lower among those assigned to a Mediterranean diet supplemented with extra-virgin olive oil or nuts than among those assigned to a reduced-fat diet.”
There are tons of “diets” out there promoting health. The DASH (Dietary Approaches to Stop Hypertension) was developed as a nutritional plan to improve blood pressure. The Traditional Mediterranean Diet (TMD) has tons of data validating its health benefits.
Then there are keto diets, Paleo, South Beach, and the list goes on and on. There may be benefits to each of these nutritional approaches but knowing what and how to eat in order to be healthy can be very confusing.
We’ve taken the main principles from diets with the best data behind them and consolidated them into this 5 step plan. We’ve also broken it up into ‘What to eat’ and ‘how much to eat’ to give you an idea of where to start. To be clear, this nutritional approach is focused on overall health and cardiovascular disease prevention. The primary focus is not necessarily weight loss and it may not be the best diet for gut health (in some people). But, this approach has excellent data for hypertension, cardiovascular disease, and overall health.
What to Eat
Step 1 – Eliminate Sugars
Cut out sugars & sweets! This is the single most important thing you can do for your health. No more than 50 grams per day and less is better. No sweetened beverages of any kind – this includes artificial sweeteners. No pastries either.
Also, be sure to eliminate High-Fructose Corn Syrup (HFCS). It isn’t natural and it isn’t good for you. Eliminate it by avoiding processed, packaged foods and sugar sweetened beverages.
Step 2 – Fix the Fat
After eliminating sugars, the next most important thing to do is clean up the fats in your diet. I believe that much of the benefit of the Traditional Mediterranean Diet is due to the focus on high quality fats.
Step 2a – Eliminate Trans-fats.
Trans-fats are evil! Thing about margarine, vegetable shortenings, and processed foods such as pastries.
Trans-fats are naturally formed by bacteria in the stomach of cattle, sheep, and goats. CLA is a natural, and healthy, trans-fat. This one is a good one!
However, the artificial trans-fats that are made in a lab or kitchen are a product of a process call hydrogenation and are horrible! Vegetable oils, through a process, have hydrogen atoms added to them creating a “partially hydrogenated” oil. These are evil. Don’t eat them. Ever!
By law, if a food contains less than 0.5 grams of trans-fats they can label them “trans-fat free.” This is very misleading because if their product contains 0.9 grams of trans-fat per serving they can simply cut the serving size in half which would drop the trans-fat levels to less than 0.5 grams and meet label claims.
The best way to eliminate trans-fat is to limit your intake of processed, packaged, or fried foods.
Step 2b – Avoid long-chain saturated fats
This includes coconut oil, butter, and cream. They may taste great but they aren’t good for your cardiovascular system.
Your cell membranes are composed of fatty acids. Saturated fatty acids pack in tightly and create a more solid, less flowing cell membrane. That is a bad thing. In this case, it is all about balance. Too much saturated fat in your diet increases CVD risk. Too little saturated fat increases risk of hemorrhagic stroke.
Step 2c – Omega-3s
Take enough of a high-quality Omega-3 fish oil to get your Omega-3 Index greater than 8%. We measure this on our labs. One of our labs uses 4.5% and another uses 8% as they use different methodologies. Either way, be sure you have good levels.
Another option is Vital Choice sardines. I have a few patients who don’t take any Omega-3 capsules but eat a can of these every day and have Omega-3 Index levels well above 8%. Vital Choice also has wild caught salmon and several other fishes as well. Their shrimp is EXCELLENT! This is where I get nearly all of my seafood.
Step 2d – Monounsaturated Fatty Acids (MUFA)
Use a high-quality Extra-Virgin Olive Oil (EVOO) abundantly for cooking & seasoning dishes. Be sure to get at least 2-4 tablespoons per day (40 grams per day) or olive leaf extract 500mg twice daily. Be sure to get your olive oil from a GOOD source. I recommend (& use) Nika’s Olive but most of the southern California varieties will be good.
The beneficial ingredient in Olive Oil is the polyphenols. Cheap olive oil blends generally do not provide enough of the polyphenols and don’t have the benefits. You’ll spend more with the good ones but don’t waste you money on junk that doesn’t provide the healthy benefits.
Step 3 – Fruits, Veggies, & Fiber
Eat 8 servings per day of vegetables and 4 servings of vegetables. This should be the foundation of your diet. Virtually every diet plan agrees that the foundation should be fruits and veggies.
Get 50 grams of mixed fiber every day. However, you will likely be getting nearly this amount if you are eating sufficient fruits and vegetables. If you aren’t getting enough then simply supplement with some additional fiber.
Pomegranate seeds – 1/4 cup 1-2 times daily. Northwest Wild Foods is a great source for these year round. 6 ounces of Pomegranate juice works as well but may temporarily increase your blood sugar.
Step 4 – Fix Electrolytes
Step 4a – Sodium
Less than 2 grams per day. To give you an idea, 1 teaspoon = 4 grams.
Step 4b – Potassium & Magnesium
5-10 grams of potassium every day. Magnesium should be 1000mg per day. Divide this up 2-4 times a day so that you are taking 250mg 4 times daily or 500mg twice daily as an example. Look for chelated forms of magnesium such as Malate, Glycinate, or Taurate. If you read the tables below, you’ll see that this diet is designed to give you more than 500mg of magnesium and 4,700mg of potassium daily so you shouldn’t need to supplement as much if you are getting appropriate nutrition.
Step 5 – Get Enough Protein
Consume 1.5g/kg of protein. The data shows that it doesn’t matter if you are eating animal sources or vegetable sources. The point is to make sure that you are getting enough. Several studies show that getting enough protein decreases blood pressure.
Focus on white meat (chicken, rabbit) and clean beef. Sources for these meats absolutely matter. Red meat is NOT a problem IF you get high-quality, natural, grass-fed sources. The problem comes in with the addition of toxins in these meats which are more common in animals grown using industrial methods (confined animal feeding operations [CAFOs]). Also, avoid processed and cured meats as well as sausage.
Eat at least 3 servings per week of fish or seafood including at least 1 serving of a fatty fish. Ideally, these meats will be the foundation of your protein.
How Much to Eat
There are numerous recommendations for how much you should eat based on a number of factors. The a common solution would be to multiply your weight in pounds by 10 and that is the number of calories to eat daily. However, I generally recommend that you cut back on calories at least 12.5% which has many health benefits.
Rule 1 – Daily calorie intake (weight in pounds x 10) x .875 (87.5%) = the number of calories to eat per day
Rule 2 – 12 Hour daily fast. Don’t eat between the hours of 6pm to 6am. Or 7pm to 7am. However you slice it is fine. Just have a 12 hour period with no calories. It changes your biochemistry for the better.
Rule 3 – get an additional 12.5% calorie deficit through exercise. For example, if you weigh 150 pounds then you should eat 1312 calories daily (cut out 188 calories). You should exercise enough to burn at least 188 calories daily.
These 3 rules change physiology and biochemistry for the better and result in a healthier & younger (physiologically speaking) you. This is a GREAT place to start!
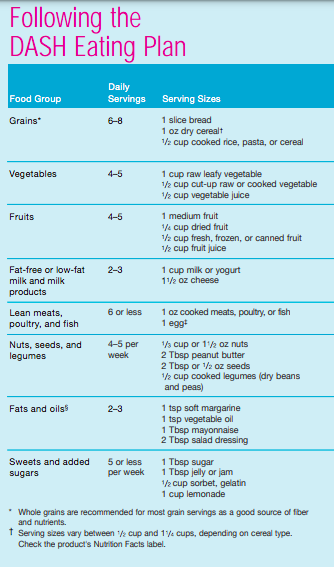
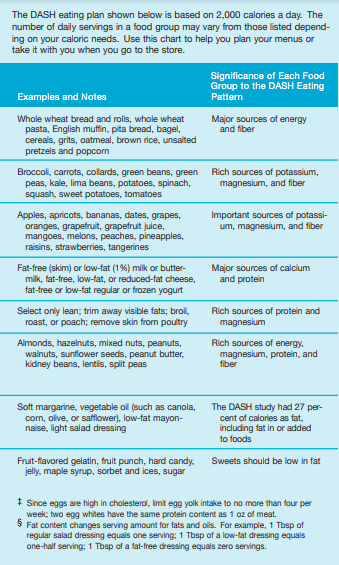
The DASH Diet followed these Daily Nutrient Goals:
Total Fat – 27%
Saturated Fat – 6%
Protein – 18%
Carbohydrates – 55%
Potassium – 4,700mg
Calcium – 1,250mg
Magnesium – 500mg
Fiber 30g
The DASH studies broke down the Daily Nutrient Goals as follows:
You can read more about the DASH diet and recommendations for it here.
This post is largely a reproduction of a report on the DASH diet. I don’t necessarily agree with all of these recommendations. These are simply the recommendations for the DASH Diet.
DASH stands for “Dietary Approaches to Stop Hypertension.”
The DASH Diet is a healthy eating plan that has been shown to reduce high blood pressure (hypertension). It may also reduce your risk for type 2 diabetes, heart disease, and stroke. The DASH eating plan may also help with weight loss.
What are tips for following the DASH Diet?
General guidelines for the DASH Diet
1) Avoid eating more than 2,300 mg (milligrams) of salt (sodium) a day. If you have hypertension, you may need to reduce your sodium intake to 1,500 mg a day.
2) Limit alcohol intake to no more than 1 drink a day for non-pregnant women and 2 drinks a day for men. One drink equals 12 oz of beer, 5 oz of wine, or 1½ oz of hard liquor.
3) Maintain a healthy body weight or to lose weight. Ask what an ideal weight is for you.
4) Get at least 30 minutes of exercise that causes your heart to beat faster (aerobic exercise) most days of the week. Activities may include walking, swimming, or biking.
5) Work with your health care provider or diet and nutrition specialist (dietitian) to adjust your eating plan to your individual calorie needs.
Reading food labels
Check food labels for the amount of sodium per serving. Choose foods with less than 5 percent of the Daily Value of sodium.
Generally, foods with less than 300 mg of sodium per serving fit into this eating plan.
To find whole grains, look for the word “whole” as the first word in the ingredient list.
Shopping
Buy products labeled as “low-sodium” or “no salt added.”
Buy fresh foods. Avoid canned foods and premade or frozen meals.
Cooking
Avoid adding salt when cooking. Use salt-free seasonings or herbs instead of table salt or sea salt. Check with your health care provider or pharmacist before using salt substitutes.
Do not fry foods. Cook foods using healthy methods such as baking, boiling, grilling, and broiling instead.
Cook with heart-healthy oils, such as olive, soybean, or sunflower oil.
Meal planning
Eat a balanced diet that includes:
5 or more servings of fruits and vegetables each day. At each meal, try to fill half of your plate with fruits and vegetables.
Up to 6–8 servings of whole grains each day.
Less than 6 oz of lean meat, poultry, or fish each day. A 3-oz serving of meat is about the same size as a deck of cards. One egg equals 1 oz.
2 servings of low-fat dairy each day.
A serving of nuts, seeds, or beans 5 times each week.
Heart-healthy fats. Healthy fats called Omega-3 fatty acids are found in foods such as flaxseeds and coldwater fish, like sardines, salmon, and mackerel.
Limit how much you eat of the following:
Canned or prepackaged foods.
Food that is high in trans fat, such as fried foods.
Food that is high in saturated fat, such as fatty meat.
Sweets, desserts, sugary drinks, and other foods with added sugar.
Full-fat dairy products.
Do not salt foods before eating.
Try to eat at least 2 vegetarian meals each week.
Eat more home-cooked food and less restaurant, buffet, and fast food.
When eating at a restaurant, ask that your food be prepared with less salt or no salt, if possible.
What foods are recommended on the DASH Diet?
The items listed may not be a complete list. Talk with your dietitian about what dietary choices are best for you.
Grains
Whole-grain or whole-wheat bread. Whole-grain or whole-wheat pasta. Brown rice. Oatmeal. Quinoa. Bulgur. Whole-grain and low-sodium cereals. Pita bread. Low-fat, low-sodium crackers. Whole-wheat flour tortillas.
Vegetables
Fresh or frozen vegetables (raw, steamed, roasted, or grilled). Low-sodium or reduced-sodium tomato and vegetable juice. Low-sodium or reduced-sodium tomato sauce and tomato paste. Low-sodium or reduced-sodium canned vegetables.
Fruits
All fresh, dried, or frozen fruit. Canned fruit in natural juice (without added sugar).
Meat and other protein foods
Skinless chicken or turkey. Ground chicken or turkey. Pork with fat trimmed off. Fish and seafood. Egg whites. Dried beans, peas, or lentils. Unsalted nuts, nut butters, and seeds. Unsalted canned beans. Lean cuts of beef with fat trimmed off. Low-sodium, lean deli meat.
Dairy
Low-fat (1%) or fat-free (skim) milk. Fat-free, low-fat, or reduced-fat cheeses. Nonfat, low-sodium ricotta or cottage cheese. Low-fat or nonfat yogurt. Low-fat, low-sodium cheese.
Fats and oils
Soft margarine without trans fats. (Doc Edwards’ note: do not eat margarine!!) Vegetable oil. Low-fat, reduced-fat, or light mayonnaise and salad dressings (reduced-sodium). Canola, safflower, olive, soybean, and sunflower oils. Avocado.
Seasoning and other foods
Herbs. Spices. Seasoning mixes without salt. Unsalted popcorn and pretzels. Fat-free sweets.
What foods are not recommended on the DASH Diet?
The items listed may not be a complete list. Talk with your dietitian about what dietary choices are best for you.
Grains
Baked goods made with fat, such as croissants, muffins, or some breads. Dry pasta or rice meal packs.
Vegetables
Creamed or fried vegetables. Vegetables in a cheese sauce. Regular canned vegetables (not low-sodium or reduced-sodium). Regular canned tomato sauce and paste (not low-sodium or reduced-sodium). Regular tomato and vegetable juice (not low-sodium or reduced-sodium). Pickles. Olives.
Fruits
Canned fruit in a light or heavy syrup. Fried fruit. Fruit in cream or butter sauce.
Meat and other protein foods
Fatty cuts of meat. Ribs. Fried meat. Bacon. Sausage. Bologna and other processed lunch meats. Salami. Fatback. Hotdogs. Bratwurst. Salted nuts and seeds. Canned beans with added salt. Canned or smoked fish. Whole eggs or egg yolks. Chicken or turkey with skin.
Dairy
Whole or 2% milk, cream, and half-and-half. Whole or full-fat cream cheese. Whole-fat or sweetened yogurt. Full-fat cheese. Nondairy creamers. Whipped toppings. Processed cheese and cheese spreads.
Fats and oils
Butter. Stick margarine. Lard. Shortening. Ghee. Bacon fat. Tropical oils, such as coconut, palm kernel, or palm oil.
Seasoning and other foods
Salted popcorn and pretzels. Onion salt, garlic salt, seasoned salt, table salt, and sea salt. Worcestershire sauce. Tartar sauce. Barbecue sauce. Teriyaki sauce. Soy sauce, including reduced-sodium. Steak sauce. Canned and packaged gravies. Fish sauce. Oyster sauce. Cocktail sauce. Horseradish that you find on the shelf. Ketchup. Mustard. Meat flavorings and tenderizers. Bouillon cubes. Hot sauce and Tabasco sauce. Premade or packaged marinades. Premade or packaged taco seasonings. Relishes. Regular salad dressings.
The DASH Diet is a healthy eating plan that has been shown to reduce high blood pressure (hypertension). It may also reduce your risk for type 2 diabetes, heart disease, and stroke.
With the DASH Diet, you should limit salt (sodium) intake to 2,300 mg a day. If you have hypertension, you may need to reduce your sodium intake to 1,500 mg a day.
When on the DASH Diet, aim to eat more fresh fruits and vegetables, whole grains, lean proteins, low-fat dairy, and heart-healthy fats.
Work with your health care provider or diet and nutrition specialist (dietitian) to adjust your eating plan to your individual calorie needs.
Pomegranate seeds for cardiovascular health are an amazing and wonderful fruit.
There are numerous reasons you should consider adding Pomegranate seeds to your diet. The problem is that they are very seasonal and not available much of the year. That makes it hard to get them all the time.
Then I came across Northwest Wild Foods who has fresh, frozen, organic pomegranate seeds. I was a bit skeptical because many of the frozen fruits I’ve had in the past, while good, just aren’t like eating the fresh stuff. Regardless, I wanted the benefits of these tasty seeds so I ordered some. I was going to start with 3 pounds. Then I saw that they had free shipping on orders over $120 so I ordered 12 pounds ($129).
That sounds like a lot of money but when you break it down they are only $0.67 per ounce. Target has them for $0.92 per ounce in smaller cups so this was actually a pretty good deal.
Once the order arrived, I opened one of the 1# bags containing the frozen arils and scooped out a serving. I was pleasantly surprised! The arils tasted fantastic frozen. Maybe my new favorite treat. Once they thawed, the consistency was pretty good. They seem to tolerate freezing better than many of the other berry fruits I’ve tried.
I highly recommend these frozen pomegranate seeds. They’ll provide a year-round source of this healthy fruit and they’ll be a staple in my freezer from now on.
Benefits of Pomegranate Seeds for cardiovascular health
As stated above, pomegranate has tremendous health benefits and has been shown to improve many cardiovascular functions. Pomegranate is rich in tannins, anthocyanins, and polyphenols.
Pomegranate has Angiotensin Converting Enzyme Inhibitor activity (ACEi). This means that it has some antihypertensive effects similar to medications like Lisinopril, Benzepril, etc. In fact, it decreases the activity of the enzyme by 36%.1
Pomegranate decreases blood pressure: systolic blood pressure (SBP) decreases 5-12% in humans (p<0.01). It decreased blood pressure 3.14/2.33 mmHg on 330 mL per day in 4 weeks in one study.
Postprandial (after meals) increase in blood pressure after a high fat meal is decreased if you consume pomegranate seeds for cardiovascular health.
Carotid Intima-Media Thickness (CIMT) is decreased 30% in 1 year with pomegranate consumption.2
oxLDL is reduced 60-90% with pomegranate consumption.2 This is huge as oxLDL is a major diving force for cardiovascular disease. Pomegranate (for 1 year) also
Increases serum Paraoxonase 1 (PON 1) 83%
LDL basal oxidative state decreased 90%
LDL susceptibility to copper ion-induced oxidation decreased 59%
Serum oxLDL antibodies decreased 19%
Serum total antidoxidant status increased by 130%
Pomegranate increases endothelial nitric oxide synthase (eNOS) as well as Nitric Oxide (NO) and improves endothelial function.
Pomegranate seeds increase enzyme antioxidants such as catalase, superoxide dismutase (SOD), and glutathione peroxidase.
In short, pomegranate seeds are anti-hypertensive, anti-atherosclerotic, anti-oxidant, and anti-inflammatory.
How much pomegranate seeds should you consume? Anywhere from 1/4 cup twice daily. Given how much I love pomegranate seeds and that I have a source year-round, I’ll be consuming at least a cup every day.
References:
Aviram m, Dornfeld L. Pomegranate juice consumption inhibits serum angiotensin converting enzyme activity and reduces systolic blood pressure. Atherosclerosis 2001;158:195(8)
Aviram M, Rosenblat M, Gaitini D, Nitecki S, Hoffman A, Dornfeld L, Volkova N, Presser D, Attias J, Liker H, Hayek T. Pomegranate juice consumption for 3 years by patients with carotid artery stenosis reduces common carotid intima-media thickness, blood pressure and LDL oxidation. Clin Nutr 2004 Jun;23(3):423-33.
Mohan M, Waghulde H, Kasture S. Effect of pomegranate juice on Angiotensin II-induced hypertension in diabetic Wistar rats. Phytother Res. 2010 Jun;24:S 196-203
Everyone should be consuming olive oil. There are tons of health benefits and lots of data supporting getting sufficient intake. Our Functional Medicine approach to health would suggest that nearly everyone should be getting good amounts of a high quality olive oil.
There is also a lot of information about poor olive oil quality, scams, and adulteration. It is major big business! I do not recommend Olive Oil purchased at Sam’s Club, Costco, and many other retailers. These blends of Olive Oil from Europe give me high concern for poor quality.
My recommendation is to get your olive oil from southern California. They maintain some of the highest standards around! The company I personally use is Nika’s Olive. They’ll ship it straight to your house. They have a bunch of different options but if you want just plain ole olive oil then go for the Arbosana Ultra Premium Olive Oil.
I recommend at least 2 tablespoons per day but it is better to go with 4 tablespoons per day, especially if you have cardiovascular issues or hypertension.
Here is how you can get your 4 tablespoons per day of Olive Oil:
drink it out of the bottle
cook with it (less than 450 degrees)
use it as salad dressing
combine it in a shake/smoothie
It doesn’t matter HOW you get it in, just get it in!
******This portion of the post is under development*******
Reduces arterial stiffness, endothelial dysfunction, and CVD.
A study of 23 hypertensive subjects in DBRCO study for 6 months – Extra virgin olive oil vs. sunflower oil
Significant reduction in blood pressure – 8/6 mmHg in hypertensive patients (P <0.05 and <0.01)
Reduces need for antihypertensive drugs in 48% of hypertensive patients vs 4% in the control group (P <0.005)
Reduces blood pressure in type-2 diabetes (clinic and 24-hour ambulatory blood pressure)
No reduction of blood pressure in normotensive or non-diabetic patients
Extra-Virgin Olive Oil reduces blood pressure
DBRC crossover study with 31 hypertensive, elderly patients
EVOO 40 grams per day vs sunflower oil for 4 wks, then 4 week washout, then 4 week crossover.
Systolic blood pressure (SBP) reduced from baseline to 136 +/- 10 mmHg with EVOO vs 150 +/- 8 mmHg with sunflower oil (P<0.01)
Seven other human clinical trials with 368 patients show similar results
The systolic blood pressure is usually reduced better than diastolic but depends on the total phenol content.
Conclusion: EVOO with a total phenol content of at least 161mg/kg at 20-40 grams (2-4 tablespoons) per day will significantly decrease blood pressure in about 3 weeks. EVOO with 300 mg/kg of total phenols may also decrease diastolic blood pressure.
Olive Oil polyphenols and blood pressure
24 women with Stage 1 hypertension (by the old standards by the way) in a double-blind, crossover study with polyphenol-rich olive oil 30mg per day for 2 months with a 4 week washout
Oleic acid and other polyphenols are responsible for BP reduction
Blood pressure reduction of 7.91/6/65 mmHg
Decreased ADMA
Decreased oxLDL
Decreased hsCRP
Increased plasma nitrates and nitrites (good for nitric oxide)
Improved FMD and endothelial dysfunction
A Mediterranean diet supplemented with extra virgin olive oil or nuts improves endothelial markers involved in blood pressure control in hypertensive women.
Serum nitric oxide (NO) reduction and increased endothelin-1 play a pivotal role in endothelial dysfunction and hypertension
Non-smoking women with moderate hypertension were submitted for 1 year to interventions promoting adherence to the TMD, EVOO, and the other with nuts versus a control low-fat diet (30 participants per group). Blood pressure, nitric oxide, and endothelin-1 and gene expression as well as oxidative stress biomarkers were measured.
Results: Serum nitric oxide and systolic blood pressure or diastolic blood pressure were negatively associated at baseline as well as between nitric oxide and Endothelin-1. Diastolic blood pressure reduction occurred with both interventions. A negative correlation was observed between changes in nitric oxide metabolites, concentration, and systolic blood pressure or diastolic blood pressure after the intervention with TMD plus extra virgin olive oil (P=0.03 and P=0.044, respectively).
Systolic blood pressure reduction was related to impairment of the serum endothelin-1 concentrations after the intervention with TMD + nuts (p = 0.008). there were also changes in endothelial nitric oxide synthase, caveolin-2, an endothelin-1 receptor Gene expression which are related to nitric oxide metabolite levels and blood pressure.
Conclusions: The changes in nitric oxide and endothelin-1 as well as endothelin-1 receptors gene expression explained, at least partially, the effect of extra virgin olive oil or nuts on lowering blood pressure among hypertensive women.
Olive oil is rich in oleic acid. It is a monounsaturated fatty acid. Extra virgin olive oil contains 5 mg of phenol’s a for every 10 g of oil. 40 g of olive oil is approximately 4 tablespoons. Olive oil increases HDL. LDL cholesterol rich oleic acid is more resistant oxidation. Replacing dietary olive oil with saturated fat significantly increases blood pressure. Olive oil is also the most resistant to oxidation.
References:
Am J Clin Nutr 2011;93:446 (also 275 & 267)
Arch IM 2000;160:837-42
Current Atherosclerosis Reports 2000;2:521-8
Diabet Med 1995;12:600-6
J Hypertens 1986;4:407-12
Arterioscler Thrmob 1992;12:911-19
J Clin Invest 1993;91:668-76
J Am Oil Chem Soc 1991;68:669-71
Clin Nutr 2004;23:1113
J Agric Food Chem 2009;57:11427
Nutr Metab Cardiovasc Dis 2010;20:284
Flynn, M and Wang S. Olive Oil as Medicine: The effect on Blood Pressure. The Report of UCD Olive Center. December 2015
Am J Hypertens 2012;25:1299
A Mediterranean diet supplemented with extra virgin olive oil or nuts improves endothelial markers involved in blood pressure control in hypertensive women. Eur J Nutr. 2015 Oct 8. [epub ahead of print]
When it comes to nutritional supplements we have to address both of these.
Are you tired of guessing when it comes to your nutrition?
Are you spending money on supplements you don’t need?
We have the solution for you!
Quality in nutritional supplements is our first priority. Many of our patients ask for a thorough nutritional evaluation. Spectracell offers a great test that evaluates the functional status of your physiology based on your nutrient status.
Chromium is an essential trace mineral that plays an important role in optimizing insulin function and the regulation of blood glucose levels. Chromium may also be anti-atherogenic and assist in lowering cholesterol. Following food intake, blood glucose levels rise causing insulin to be secreted by the pancreas. Insulin lowers blood glucose levels by increasing the rate at which glucose enters a person’s cells. Chromium is believed to facilitate the attachment of insulin to the cell’s insulin receptors. Studies also indicate that chromium participates in cholesterol metabolism, suggesting a role for this mineral in maintaining normal blood cholesterol levels and preventing atherosclerosis. Chromium also plays a role in nucleic acid synthesis.
Deficiency Symptoms:
Due to processing methods that remove most of the naturally occurring chromium from commonly consumed foods, dietary deficiency of chromium is believed to be widespread in the United States. Chromium deficiency may increase the likelihood of insulin resistance, a condition which the cells of the body do not respond to the presence of insulin. Insulin resistance an lead to elevated blood levels of insulin (hyperinsulinemia) and elevated blood levels of glucose, which can ultimately cause heart disease and/or diabetes. Deficiency of chromium is associated with metabolic syndrome. Metabolic syndrome represents a constellation of symptoms, including hyperinsulinemia, high blood pressure, high triglyceride levels, high blood sugar levels, and low HDL cholesterol levels. These symptoms increase one’s risk for heart disease. Low levels of chromium are also associated with an increased risk of coronary artery disease incidence and mortality.
Chromium deficiency correlate with depressed nucleic acid synthesis. Chromium is essential for maintaining the structural stability of proteins and nucelic acids and animal studies have found that this element is also vital for healthy fetal growth and development. Studies on humans have established that premature infants and those with evidence of intrauterine growth retardation have significantly lower chromium status compared to infants born full-term. Others have found that multiparous women have far lower body chromium levels compared to nulliparous women. These findings suggest that chromium is an essential trace element during fetal growth and development.
Repletion Information:
In 2001, the Institute of Medicine at the National academy of Sciences conducted a thorough review of the chromium research can concluded that excessive intake of chromium from foods or supplements is not associated with any adverse effects. As a result, to Tolerable Upper Intake Level (UIL) was established for this mineral. However, people with liver or kidney disease may be more susceptible to adverse effects from excessive intake of chromium, and such individuals are cautioned to avoid taking more than 200 micrograms of chromium supplements per day. There is limited evidence to suggest that long-term chromium picolinate supplementation at levels greater than 200 micrograms per day may also be hazardous to chromosome integrity and should be avoided.
Vitamin A is actually a family of similar compounds, the retinoids, that are related to retinol. Apparently, retinoic acid performs most of the functions of vitamin A, binding to DNA receptors in target cells. You can see the diagram of this and it might make more sense.
There are 4 biologically important retinoids:
Retinol– the alcohol form. Retinol esters are packaged into chylomicrons and transported to the liver for storage. When retinol is released from the liver, it complexes with retinol binding protein (RBP) and is delivered to target tissues throughout the body (except heart and skeletal muscle). In the cytosol, retinol is irreversibly oxidized to retinoic acid (similar to steroid hormones) which binds to nuclear receptors forming a complex which activates gene transcription of protein products .
Retinal– the oxidized form of retinol. The two are readily convertable. Retinal is a component of the visual pigments within rod and cone cells of the retina (see below).
Retinoic Acid– the oxidized form of retinal. It cannot be reduced in the body. Thus, it cannot give rise to retinol or retinal. It has wide pharmacologic therapies in dermatology.
b-carotene– plant form of vitamin A. Oxidatively cleaved (via thyroid hormone) in the intestine to 2 molecules of retinal. Unfortunately, this conversion process is inefficient and the vitamin A activity of b-carotene is only about 1/6 that of retinol.
RDA: for adults- 1000 retinol equivalents (RE) for males and 800 RE for females. One RE=1 mg of retinol; 6 mg of b-carotene; or 12 mg of other carotenoids.
Good sources of Vitamin A: liver, kidney, cream, butter, and egg yolks have pre-formed vitamin A. Yellow and dark green vegetables and fruits are good sources of carotenes.
Functions of Vitamin A: The functions of vitamin A can be divided into four categories.
Visual Cycle- see this in the diagram below.
Growth- Absence of vitamin A prevents bone growth from keeping up with the growth of nervous tissue and can lead to CNS damage. Also, there is a hyper-keratinization of the taste buds on the tongue which decreases the person’s appetite (at first anyway).
Reproduction- prevents fetal resorption in the female and supports spermatogenesis in the male. Retinoic acid doesn’t help here or with the visual cycle. Therefore, if anyone has only had retinoic acid since birth, they are blind and sterile.
Maintenance of Epithelial Cells- you gotta have this stuff for epithelial differentiation and mucous secretion.
active forms of vitamin A are used in the treatment of skin disorders and acute progranulocytic leukemia (M3)
• topical tretinoin (all-trans-retinoic acid) is used in the treatment of psoriasis and mild acne
• oral isotretinoin is used to treat severe acne, however, it is teratogenic, so women must have a pregnancy test before it is prescribed and must be placed on birth control pills for the full duration of therapy 0 is used to treat acute progranulocytic (promyelocytic) leu emia (M3) and is thought to induce maturation of the leukemic cells
Retinoic acid as a pharmacotherapeutic- effective treatment of acne and psoriasis. Everything I have seen states that you have to use an all trans retinoic acid (tretinoin) which is too toxic for systemic use and must only be applied topically. However, if the pt doesn’t respond to this therapy, and if they have a severe case, you can use isotretinoin (13-cis retinoic acid) orally.
b-carotene- Populations that consume increased amounts of b-carotene also have a reduction in heart disease and lung and skin cancer. These effects are independent of b-carotene being a precursor to vitamin A and probably due to its antioxidant effects (see oxidative damage). b-carotene, unlike vitamin A, is not toxic even at high doses.
Toxicity: Some would argue that this can be the most toxic of the vitamins. You shouldn’t exceed 7.5 m. An excess of b-carotenes in the diet turns the skin yellow, however, the sclera remain white and signs of vitamin A toxicity do not occur
Deficiency Symptoms: Night blindness (nyctalopia), xerophthalmia (dryness of the cornea & conjunctiva – can lead to blindness), dry-rough skin, follicular keratosis, bronchogenic carcinoma (squamous metaplasia may progress to dysplasia & cancer), poor wound healing, & impaired bone growth. Vitamin A deficiency is the most common deficiency in the world and the 2nd leading cause of blindness (second only to Chlamydia trachomatis).
The active form of thiamine is thiamine pyrophosphate (TPP) which is essential for the conversion of pyruvate to acetyl CoA and Step 4 of the Kreb’s cycle. It is also essential for the conversion of glyceraldehyde-3-phosphate (one of the glycolysis intermediates) to ribose-3-phosphate.
Good sources: Sunflower seeds, liver, pork, whole and enriched grains, and dried beans. According to one source, the outer layer of seeds is high in thiamine. Thus, whole wheat breads are high in thiamine while bread made from milled grain is low in thiamine.
DRI: 0.9-1.2 mg per day
Functions: the functions of this vitamin are listed above. It also assists in nerve function.
Cofactor to over 24 enzymes
Essential to the production of energy from food in the form of ATP (adenosine triphosphate)
Cofactor to pyruvate dehydrogenase (for energy production in Krebs cycle)
Cofactor in the maintenance of myelin sheath (nerve cell insulator)
Activates membrane ion channels which affect nerve and muscle cell function
Cofactor to transketolase for fat, protein and carbohydrate metabolism
Cofactor to transketolase for synthesis of ribose for incorporation into DNA (deoxyribonucleic acid)and RNA
Cofactor to transketolase for synthesizing cellular NADPH (Nicotinamide Adenine DinucleotidePhosphate Hydrogen) used for fatty acid biosynthesis
Cofactor to 2-oxo-glucarate dehydrogenase (also called α-ketoglutarate dehydrogenase) whichmakes acetylcholine, gamma amino butyric acid (GABA) and glutamate
Cofactor to α-ketoglutarate dehydrogenase for mitochondrial energy production
Cofactor to branched chain ketoacid dehydrogenase for mitochondrial energy production
Cofactor in the hexose monophosphate shunt, an anabolic pathway used by certain cells
Cofactor to glucose metabolism, particularly in central nervous system
Cofactor in the mitochondrial respiratory chain
Deficiency impairs oxidative metabolism leading to increased pyruvate and lactate, which cancause vasodilation, retention of water and contribute to heart failure (“cardiac or wet beriberi”)
Some cardiac medication decreases vitamin B1 uptake in myocytes (muscle cell)
Deficiency in children linked to delayed language development
Supplementation may benefit autistics
Supplementation may benefit inborn errors of metabolism of branched chain amino acids such as thiamin responsive branched chain ketoaciduria (also known as maple syrup urine disease)
Regulates intracellular p53 activity (a protein that protects against tumors)
Deficiency may cause serotonin depletion which can decrease pain threshold, decrease musclerepair enzymes (muscle soreness) and poor energy production (fatigue)
Key role in restorative sleep
Plays a role in acetylcholine production in the brain
Plays a role in nerve impulse conduction
Conversion of thiamin to biologically active form requires magnesium
Sulfites in food destroy vitamin B1
Excess alcohol inhibits activation of thiamine coenzymes
Deficiencies:Beri-Beri which means “I can’t, I can’t.” Infantile beri-beri symptoms include: tachycardia, vomiting, convulsions, and death. Adult beri-beri symptoms are: dry-skin, irritability, disorderly thinking, and progressive paralysis. Alcoholics are particularly at risk for thiamine deficiency for two reasons. First of all, they are likely to have a reduced intake and, secondly, alcohol decreases thiamine absorption.
Toxicity: Thiamine is not considered toxic. However, some have linked headaches and insomnia to thiamine when their doses exceeded 5 mg/d for 4-5 wks.
Riboflavin is needed for the formation of flavin mononucleotide (FMN, seen in Complex I of the ETS) and flavin adenine dinucleotide (FAD, from Step 6 of the Krebs). Below is a diagram that shows their structures.
Riboflavin is light-sensitive! That’s why you won’t see milk in a clear bottle or container.
Good sources: Milk, eggs, liver, green leafy veggies, and whole & enriched grains.
DRI: 0.9-1.3 mg per day
Functions: The 2 co-enzymes discussed above (FMN and FAD).
All known functions:
Essential to the production of energy from food in the form of ATP (adenosine triphosphate)
Active form is FAD (flavin adenine dinucleotide) and FMH (flavin mononucleotide, also calledriboflavin 5’-phosphate) which are cofactors for oxidation-reduction reactions in energy production
FAD assists methylation reactions throughout body
Coenzymes derived from riboflavin are called flavins
Enzymes that use a flavin coenzymes are called flavoproteins
Flavins metabolize drugs and toxins
Low B2 can impair methylation reactions in the brain, which may present clinically as depression
Activates glutathione reductase, which regenerates the antioxidant glutathione
Key role in iron utilization
Aids in mobilization of ferritin from tissues; helpful for anemia
FAD is a cofactor for methylenetetrahydrofolate reductase (MTHFR) so for people who arehomozygous for 677C→T MTHFR gene, riboflavin may lower their homocysteine
Recycles folate into a usable methyl-donor form (converts 5,10-methylene TH4-folate to 5-methylTH4-folate)
People with 677C→T MTHFR gene tend to respond well to B2 therapy to lower blood pressure
Cofactor to xanthine oxidase, which synthesizes uric acid and aids in purine catabolism
Cofactor to pyridoxal 5’-phosphate oxidase, which converts vitamin B6 into its active form
Cofactor in the conversion of retinol (vitamin A) to retinoic acid
Cofactor to kynurenine mono-oxygenase, which converts tryptophan into niacin containing enzymesNAD and NADP
Cofactor to NAD(P):quinine oxidoreductase which aids in detoxification and chemoprevention
Cofactor to protoporphyrinogen oxidase which synthesizes hemoglobin
Cofactor to dihydrolipoyl dehydrogenase which aids energy metabolism
Cofactor to fatty acyl-CoA-dehygrogenase which aids in fatty acid oxidation
Cofactor to succinate dehydrogenase which is used in the Krebs cycle for energy production
Cofactor to NADH dehydrogenase (also called ubiquinone oxidoreductase) which functions inmitochondrial respiration
Cofactor to sphinganine oxidase which synthesizes sphingosine (component of nerve tissue)
Cofactor to monoamine oxidase which aids in metabolism of several neurotransmitters such asserotonin, melatonin, epinephrine and norepinephrine
Role in mitochondrial energy metabolism may explain its efficacy in migraine prophylaxis
Role in glutathione reductase implicates riboflavin deficiency in cataract formation
Minimizes pain associated with inflammation
Augments the antinociceptive (painkiller) effects of morphine
Good sources: meats, liver, nuts, whole and enriched grains. Some niacin can be synthesized from tryptophan (inefficient).
DRI: 12-16 mg/d
Functions: Co-enzyme formation (NAD+ and NADP), fatty acid metabolism, and decrease serum cholesterol. It is the most potent agent to increase serum HDL at doses 100 times the RDA (but many people can’t tolerate the side effects). It does this by strongly inhibiting lipolysis in adipose tissue, which is the largest producer of circulating FFA’s. Decreased FFA’s are needed for the formation of VLDLs. LDLs are produced from VLDLs. Thus, niacin inhibits the formation of LDLs (indirectly). It is especially useful for the treatment of type IIb hyperlipidemia (both VLDL and LDL levels are increased).
Also called nicotinic acid or niacinamide or nicotinamide (not related to nicotine found in tobacco)
Nicotinic acid & niacinamide have identical vitamin properties but are different pharmacologically
Around 200 enzymes require niacin derived NAD or NADP enzymes (also called coenzyme I and
coenzyme II) usually for redox reactions
Coenzyme for NAD (nicotinamide adenine dinucleotide) and NADP (nicotinamide adenine
dinucleotide phosphate) which is needed to metabolize food
Increases the rate of NAD synthesis
NADP regenerates glutathione
Cofactor in the mitochondrial respiratory chain
NAD catabolizes carbohydrates, proteins, fats and alcohol
Cofactor to mitochondrial aldehyde dehydrogenase which metabolizes alcohol
Cofactor to glucose-6-phosphate 1-dehydrogenase which metabolizes glucose in red blood cells
Cofactor to dihydropteradine reductase which is involved in dopamine and serotonin synthesis
NADP synthesizes fatty acids and cholesterol
Only nicotinic acid influences blood lipid levels
Increases HDL (high density lipoprotein)
Lowers triglycerides by inhibiting diacylglycerol acyltransferase-2 (enzyme that synthesizes
triglycerides in liver)
Cofactor to long-chain-3-hydroxyacyl-CoA dehydrogenase which metabolizes fat for energy
Down regulates vascular cell adhesion molecules (VCAM)
Inhibits the oxidation of LDL (low density lipoproteins)
Decreases the highly atherogenic Lp(a) by reducing its rate of synthesis in the liver
Shifts lipoproteins from small, dense (atherogenic) to large, buoyant (non atherogenic)
Inhibits vascular inflammation and improves endothelial function independent of effect on lipids
Supresses cytokine-mediated induction of nitric oxide synthase, thus decreasing inflammation
Cofactor in mono-ADP-ribosyltransferase, which plays a role in cell signaling
Cofactor in poly-ADP-ribose polymerase (PARP), which aid in DNA replication and repair
Cofactor in ADP-ribosyl cyclase, which initiates release of calcium ions from inside cell
Maintains proper methylation of PARPgenes that suppress tumor formation and growth
Influences cellular response to DNA damage (cancer prevention)
Extends lifespan of human cells in vitro
Slows telomere attrition rate by reducing reactive oxygen species in mitochondria
Mediates cell signaling pathways important to the prevention of cancer
Regulates p53 activity in cells (a protein that protects against tumors)
Protect pancreatic beta cells in type 1 diabetics although high doses may impair glucose tolerance
Precursor to glucose tolerance factor which facilitates insulin binding
Pharmacological doses may enhance calming effect of GABA (gamma aminobutyric acid) in brain
Pharmacological doses may exacerbate gout or cause hepatotoxicity (liver damage)
Inhibits the enzyme tryptophan pyrrolase which breaks down tryptophan in the liver
Increases conversion of tryptophan to serotonin
Increases REM (rapid eye movement) sleep
Improves quality and quantity of sleep via its role in serotonin synthesis
Dilates blood vessels (may alleviate migraine)
Severe deficiency can cause anxiety
Increases adiponectin (weight loss hormone secreted by fat cells)
Niacin-bound chromium may help reduce body weight
Deficiencies: Clinical signs of early niacinamide deficiency include anorexia, muscular fatigue, indigestion, depression, insomnia, headaches, glossitis and skin lesions. Severe deficiency may lead to pellagra, with dermatitis, dementia, diarrhea (the 3 D’s of pellagra), tremors and sore (black) tongue. Deficiencies of thiamin, riboflavin and pyridoxine commonly accompany (or can cause) niacinamide deficiency.
Toxicity: Histamine reaction at doses >35 mg. Facial flushing is one of the symptoms of this.
It means “It’s everywhere.” Apparently they named it this because it can be found in a number of sources.
Good sources: Liver, broccoli, and egg yolks.
DRI: 4-5 mg/d. No RDA has been set.
Functions: It is the precursor to Co-enzyme A (CoA) as in acetyl CoA or succinyl CoA (see glycolysis or Kreb’s cycle).
Component of coenzyme A and acyl carrier protein (ACP), which facilitates metabolism of two- carbon units (acetyl groups) in the Krebs cyle
Coenzyme A is a cofactor in over 70 enzymatic pathways
ACP is cofactor to fatty acid synthase, which is required for fatty acid elongation
Essential to the production of energy from food in the form of ATP (adenosine triphosphate) via itsrole in transfer of acetyl groups for the metabolism of carbohydrates, fats and proteins
Acetyl groups are involved in synthesis of cholesterol, steroid hormones, porphyrin (hemoglobin), phospholipids (cell membranes)
Coenzyme A is involved in coenzyme Q10 synthesis
Coenzyme A is needed for prostaglandin synthesis
Coenzyme A is needed for acetylcholine synthesis
Coenzyme A is needed for melatonin synthesis
Coenzyme A is needed for pyruvate degradation
Coenzyme A is required for phase II detoxification of xenobiotics and several drugs by the liver
ACP is needed for sphingolipid production, makes the myelin sheath around nerves
Modulates protein structure, gene expression and cell signaling via coenzyme A activity
Increases activity of lipoprotein lipase, an enzyme that breaks down fat cells
May reduce hunger during calorie restriction
Modifies action of several enzymes involved in cholesterol synthesis
Favorably alters LDL (low density lipoprotein) metabolism to less atherogenic type
Functions: Biotin is required for proper metabolism of fats and carbohydrates. Biotin-dependent enzymes catalyze the addition of carboxyl groups (COO-) from bicarbonate, for use in fatty acid biosynthesis, gluconeogenesis, lipogenesis, propionate metabolism and leucine catabolism. Biotin is a co-enzyme in glucose production and fat synthesis.
Cofactor Functions:
Cofactor to acetyl-CoA carboxylase, needed for fatty acid metabolism
Cofactor to pyruvate carboxylase, an enzyme needed for gluconeogenesis
Cofactor to methylcrotonyl-CoA carboxylase, which metabolizes leucine
Cofactor to propionyl-CoA carboxylase (also called holocarboxylase synthetase), which metabolizes amino acids and cholesterol
Cofactor for fatty acid synthesis (specifically for elongating the fatty acid chain)
All Other Functions:
The protein in egg whites (avidin) binds to biotin preventing its absorption so those who consume raw egg are at increased risk of biotin deficiency
Essential cofactor for four carboxylase enzymes in the mitochondria
Common indications of biotin deficiency include brittle nails, alopecia and dermatitis due to impaired fatty acid synthesis from reduced biotin-dependent carboxylases enzymes (particularly acetyl-CoA carboxylase)
Decreases synthesis of cytokines (interleukin-1 b and interleukin-2)
Decreases proliferation of peripheral blood mononuclear cells
Affects gene transcription (over 2,000 biotin dependent genes have been identifies)
Biotin deficiency in pregnancy may be teratogenic
Stimulates glucose-induced insulin secretion in pancreatic beta cells
Induces glucokinase, an enzyme needed for cells to use glucose
Accelerates glycolysis in liver and pancreas
Studies indicate in can reduce triglycerides and improve glycemic control
Biotin deficiency has induced depression in animal and human studies
Animal studies show induced biotin deficiency presents clinically as fatigue
Reduces blood pressure by activating the enzyme guanylate cyclase which in turn activates cGMP (cyclic guanosine monophosphate)
Anticonvulsant therapy such as phenobarbital and valproic acid may induce biotin deficiency
Deficiencies: Symptoms of biotin deficiency include erythematous exfoliative dermatitis, thinning hair, fatigue, irritability, mild depression, somnolence, muscle pains, anorexia, nausea, mild anemia. Infants with seborrheic dermatitis, Leiner’s disease or alopecia may indicate a biotin deficiency, along with symptoms of ketoacidosis, poor feeding, vomiting, lethargy, coma and developmental retardation. Dietary symptoms include fatigue, dry skin, body hair loss, nausea, loss of appetite and mild depression.
Those at risk for biotin deficiency include: persons consuming excessive amounts of raw egg whites, inherited disorders of biotin metabolism, extended total parenteral nutrition (biotin-free), loss of enteric gut microflora from antibiotic
therapy or altered gut motility, pregnant and lactating women, antiepileptic drug therapy, alcoholics, trauma (burns and surgery), elderly, malabsorption (especially achlorhydria).
Vitamin B6 is actually composed of a group of chemicals: pyridoxine, pyridoxal, and pyridoxamine. Pyridoxine is found in plants and the other two are found mainly in animals. Pyridoxal phosphate is the biologically active co-enzyme.
DRI: 1-1.7 mg/d. However, the requirement for pyridoxine goes up when you have a high protein intake.
FUNCTIONS: Vitamin B6 is needed to metabolize proteins and is important for a healthy immune system, nerves, bones and arteries. Vitamin B6 is a complex of three similar molecules: Pyridoxine, Pyridoxal and Pyridoxamine. All are present in foods and converted into pyridoxal-5-phosphate, the most active coenzyme form. The primary functions of vitamin B6 are in protein metabolism, transferring amino acid and sulfur groups. Roles in synthesis of heme (for hemoglobin), niacin, neurotransmitters, connective tissues, eicosanoids and sphingolipids in nerve sheaths are also essential. Vitamin B6 also participates in the utilization of glycogen and immune function.
Cofactor Functions:
Cofactor to 112 known enzymes
Cofactor for dopa decarboxylase which converts L-dopa to dopamine and 5HTP to serotonin
Cofactor to alanine-glyoxalate aminotransferase which converts glyoxylate to glycine
Cofactor to erythrocyte alanine aminotransferase which transfers amino groups
Cofactor to aspartate aminotransferase which moves amino groups between aspartate & glutamate
Cofactor to glycogen phosphorylase which releases glucose from glycogen
Cofactor to ornithine aminotransferase which makes proline & prevents gyrate atrophy (retinal degeneration)
Cofactor to glutamic acid decarboxylase that converts glutamate to the neurotransmitter GABA
Cofactor in the utilization of selenium (disconnects selenium from selenoproteins for use in the body)
Conversion to PLP is vitamin B2 dependent; Deficiency of B2 impacts B6 function
Cofactor in the synthesis and function of several neurotransmitters including serotonin, gamma-amino-butyric acid (GABA), dopamine, epinephrine and norepinephrine
Cofactor in mitochondrial respiratory chain to produce energy via ATP (adenosine triphosphate)
Cofactor to enzymes that converts homocysteine to cysteine (cystathionine synthase and cystathionase)
Cofactor in the synthesis of taurine
Cofactor in the synthesis of heme (hemoglobin)
Cofactor in the metabolism of vitamin B3 (niacin) from tryptophan via kynurenine pathway
Cofactor in the synthesis of connective tissue and eicosanoids
Cofactor in the synthesis of sphingolipids for nerve cell insulation
Cofactor in the synthesis of antibodies (key role in immune function)
Cofactor for tyrosine decarboxylase, which catalyzes the conversion of tyrosine to tyramine
Cofactor to lysyl oxidase which builds arterial integrity via role in collagen and elastin structure
Cofactor to aminolevulinic acid synthase which aids in hemoglobin synthesis
Cofactor to serine hydroxymethyltransferase which transfers methyl groups from serine to folate and initiates immune cell proliferation
Cofactor to serine palmitoyltransferase which makes sphingolipids for nerve cell insulation
Cofactor to serine facemase which synthesized neurotransmitter D-serine
Cofactor to sphinosine-1-phosphate lysase which makes sphingolipids for nerve cell insulation
Cofactor to cystathionine-b-synthase which metabolizes homocysteine and serine to form cystathionine
Cofactor or kynureninanse which metabolizes tryptophan into vitamin B3 for NAD cofactors
Cofactor to GABA aminotransferase which breaks down GABA
Cofactor to diamine oxidase, which catabolizes exogenous histidine in the gut
Cofactor for histidine decarboxylase which converts histidine to histamine
All Other Functions:
B6 is a complex of three molecules: pyridozine, pyridoxal, and pyridoxamine which are all converted to pyridoxal-5-phosphate (PLP), the active coenzyme form
Bins with histamine and inactivates it (may mitigate allergic response in asthma)
Increases peripheral metabolism of levodopa (l-dopa) making it less available for uptake into the brain (may diminish effectiveness of l-dopa medication for Parkinson’s patients when not given with carbidopa which is a peripheral decarboxylase inhibitor)
High dose B6 can be as effective as Ritalin for ADHD due to its effect of increasing serotonin
Synergistic effect with magnesium for autism patients
Increases intracellular uptake of magnesium and vice versa
Low B6 linked to high CRP (C-reactive protein), a marker of inflammation
Supplementation suppresses pro-inflammatory cytokines such as IL-6 and TNF-a
Tissue specific depletion of B6 occurs during inflammation
Crucial for DNA methylation thus regulating gene expression
Deficiency impairs conversion of alpha-linolenic acid to EPA and DHA
Protects genes from estrogen-induced damage (detoxifies estrogen) lowering risk of hormone related cancers
Regulates sex hormones and binds to steroid hormone receptors, thus decreasing their effects
Reduces prolactin levels which stimulates hypothalamus to increase testosterone
Inhibits pituitary (and other tissue) tumor proliferation via role in apoptosis (programmed cell death)
DEFICIENCIES: Convulsion, nausea, flaky skin, HA, insomnia (uncommon). Isoniazid can induce a deficiency, so you have to supplement with isoniazid prescription. Deficiency is rare but has been seen in infants with low intake of B6, females on OCP’s, and alcoholics.
Early vitamin B6 deficiency symptoms are primarily peripheral neuropathy, weakness, irritability, depression, insomnia and anxiety. More severe deficiency leads to dermatitis, nausea, vomiting and convulsions. Carpal tunnel syndrome,
premenstrual tension syndrome and atherosclerosis may also be related to vitamin B6 deficiency. Sideroblastic anemia is indicative of vitamin B6 deficiency. Homocysteine levels in serum may be elevated by a vitamin B6 deficiency.
TOXICITY: Nerve damage (it is the most toxic water soluble vitamin) @ doses > 200mg. Substantial improvement, but not complete recovery, occurs when the vitamin is removed. Another source indicated neurologic symptoms at doses of 2 grams/d.
GOOD SOURCES: Green leafy veggies, liver, lima beans, and whole grain cereals
DRI: 300-400 mg/d (0.3-0.4 mg/d); for women who are on birth control pills, this increases dramatically. After stopping BCPs, they must take 800 mg/d for at least 30 days before getting pregnant.
FUNCTIONS: Folic acid is essential for the biosynthesis of the purines and the pyrimidine , thymine.It is converted to tetrahydrofolic acid (THF) which is the biologically active form. THF receives one-carbon fragments from donors (ie. serine, glycine, & histidine) and transfers them to intermediates in the synthesis of amino acids and the nucleotides mentioned above. See the diagram below.
All Nutrient Functions:
High stomach pH (low stomach acid) decreases folic acid absorption
Needed for the production of red blood cells
Needed for the synthesis of nucleic acids
Key role in one carbon metabolism (methylation reactions) as it accepts & donates methyl groups
Precursor to SAMe (S-adenosylmethionine)
Influences telomere length via DNA methylation
Cofactor in the metabolism of methionine, histidine, tryptophan, glycine, serine, and formate
Required for the conversion of homocysteine into methionine
Affects noradrenaline and serotonin receptors in the brain
Inhibits NMDA receptors
Building block in synthesis of serotonin, dopamine, and norepinephrine
Low folate causes poor response to anti-depressant medications
Improves response to the anti-depressant drug fluoxetine
The lower the folate, the more severe the depression in some individuals
May improve response to erectile dysfunction meds (PDE5 inhibitors)
Cofactor in mitochondrial respiratory process
Improves endothelial function
Increases nitric oxide (NO) production in vascular endothelial cells
Cofactor to enzyme nitric oxide synthase
Enhances the availability of nitric oxide cofactors such a tetrahydrobiopterin
Improves flow mediated dilation
Lowers risk of colonic neoplasia in patients with ulcerative colitis
Rapidly dividing cells are the most vulnerable to folate deficiency
Alcohol interferes with the absorption and metabolism of folate
Methotrexate (cancer, arthritis, and psoriasis drug) is a folate antagonist
Individuals with homozygous C–> T in the C677T MTHFR (methylene tetrahydrofolate reductase) gene have higher folate requirements that those without two copies of this gene
Synthesis of active form of folic acid requires B2, B3, B6, zinc, Vitamin C and serine
Folate supplementation may increase Vitamin B12 requirements or aggravate neurological symptoms stemming from B12 deficiency
DEFICIENCIES: Folic acid deficiency is probably the most common vitamin deficiency in the U.S. (especially amoung pregnant females and alcoholics). Deficiency is manifested two ways: the first is Megaloblastic anemia because there isn’t enough synthesized nucleotides; the second is developmental abnormalities of the neural tube in the fetus.
The anemia is due to diminished synthesis of purines and thymidine. Therefore, the erythropoeitic cells are not able to make DNA or divide. Vitamin B12 deficiency can also cause this disorder (but at a different step). Make sure to evaluate the exact cause of megaloblastic anemia before instituting therapy. Deficiency can be brought on by increased demand (as in pregnant or lactating women), poor absorption, alcoholism, or medications (that inhibit dihydrofolate reductase such as methotrexate).
Neural tube development of the fetus is critically dependant on folic acid. Women considering getting pregnant should ensure intake of 0.4 mg/d. This amount must be consumed early because the neural tube develops very early in development (before most women know that they are pregnant). Supplementation should not exceed 1 mg/d to avoid complicating a vitamin B12 deficiency.
Deficiency Functions:
Deficiency causes neural tube defects such as spina bifida and cleft palate in newborns
Deficiency linked with cancers, especially colon and breast, although excess supplementation of folic acid has been linked with cancer cell proliferation and estrogen-related breast caner
Deficiency reduces estrogen and circulating testosterone
Deficiency alters cholinergic metabolism in the brain
Deficiency reduces proliferation of lymphocytes
TOXICITY: Masks vitamin B12 deficiency (mainly in elderly)
In contrast to the other water soluble vitamins, cobalamin is stored in the body (~4-5 mg).
There are 2 primary forms with which most people supplement: cyanocobalamin and methylcobalamin. Hydroxycobalamin is a stable form that is converted to the active, methylcobalamin form.
How it absorbs
When taken orally, Vitamin B12 binds to intrinsic factor which is produced in the stomach. The complex of Vitamin B12 & intrinsic factor is absorbable. Without intrinsic factor we cannot absorb Vitamin B12 through the gastrointestinal tract.
This issue is the most common reason that people don’t have adequate levels. We also commonly see deficiency in vegetarians and vegans because there are not good plant sources of B12.
Autoimmune attack of the gastric parietal cells destroys the bodies ability to produce intrinsic factor.
The B12-Intrinsic Factor complex is absorbed in the ileum of the small intestine. Some people may also have a gut disorder that could decrease the absorption of B12.
Good sources
This vitamin is not found in plants! It is synthesized only by microorganisms. Animals obtain cobalamin from intestinal flora or by eating the meats of other animals. Especially liver, whole milk, eggs, oysters, fresh shrimp, pork, and chicken.
DRI: 1.8-2.4 mg/d
Our sublingual methylcobalamin is 2.5mg per day and also contains 5-MTHF 1mg. We also give methylcobalamin as an injection and it is included in several of our IV nutritional formulas.
Functions:
Vitamin B12 (cobalamin) is essential for 2 enzymatic reactions: synthesis of methionine and isomerization of methylmalonyl CoA that arises from odd fatty acid chains. Cobalamin converts some forms of TetraHydroFolate (THF) to the active form (5-MTHF). If cobalamin is deficient, the inactive forms build up and cannot be converted. Therefore, cobalamin deficiency can resemble folic acid deficiency and vice versa. This process is further discussed on the Methylation post.
Repletion improves treatment response in depression
Inhibits proliferations of malignant cells in vivo
May enhance efficacy of methotrexate
Protects retinal neurons against N-methyl-D-aspartate receptor mediated glutamate neurotoxicity
Deficiencies:
Pernicious anemia. Deficiency is most often due to an inability to absorb the vitamin rather than an inadequate amount in the diet. Vitamin B12 deficiency can also lead to CNS symptoms. Folic acid supplementation can correct the anemia associated with vitamin B12 deficiency but not the CNS effects. Make sure you know which is deficient!
Deficiency causes excess methylmalonic acid which decreases fatty acid synthesis for nerve cells.
Toxicity: None known
I often look at methylcobalamin as a ‘litmus test’ of the quality of nutritional supplements. It is slightly more expensive to produce so it helps me to understand how important quality may be to the manufacturer. I only recommend methylcobalamin, adenosylcobalamin, or hydroxycobalamin supplementation whether it be orally or injectable. Most traditional doctors use the cyanocobalamin version in their ‘B12 injections.’
Cyanocobalamin has a cyanide molecule attached to it. Do you want to inject your body with cyanide?
We recommend a supplement with B12 (methycobalamin) in a sublinqual form. Sublinqual forms are absorbed directly into the blood system so we don’t have to worry about intrinsic factor and gut health for absorption.
Vitamin B12 refers primarily to cyanocobalamin (they are used interchangeably), but also to several other cobalamins which possess similar nutritional properties. Vitamin B12 is synthesized by bacteria and is found in soil and in contaminated water. The average Western diet contains 5 to 15 μg/day of vitamin B12, and exceeds the recommended dietary allowance of 2 μg/day.1,2 The primary dietary sources of vitamin B12 are in foods of animal derivation (meat, eggs, and milk). Absorption of vitamin B12 occurs when it is bound to intrinsic factor from the stomach parietal cells.2 Vitamin B12 deficiency is rare in individuals who consume animal products unless there is an underlying vitamin B12 malabsorption condition. Strict vegetariansand babies of mothers who are strict vegetarians are at an increased risk for developing anemia.1-3 The body stores a large amount of vitamin B12 (i.e., 2-5 mg), primarily in the liver. It takes 2 to 5 years to develop a vitamin B12 deficiency even in the presence of severe malabsorption.1,2 However, it is estimated that 5% to 40% of the elderly population have B12 deficiency,4 probably due to reduced intrinsic factor production.2,5
Clinical Interpretation
Vitamin B12 deficiency, related to poor intestinal B12 absorption or dietary deficiency, is associated with pernicious anemia, cardiovascular disease, cancer, and neurodegenerative disorders.6 A cobalamin-dependent reaction involves the synthesis of methionine from homocysteine using methylcobalamin as a cofactor. One hypothesis is that this reaction has primary importance in vitamin B12 and folate deficiencies. A deficiency of either vitamin impairs tetrahydrofolate production.7 In megaloblastic anemia patients, this causes a defect in DNA synthesis that prevents cell division in the marrow. RNA synthesis and cytoplasmic component synthesis are not affected, which results in the production of large erythrocytes.1,2 In addition, a deficiency of either vitamin will result in homocysteine accumulation.1
A cobalamin deficiency may also cause increased methylmalonyl-CoA and its hydrolysis product, methylmalonic acid (MMA).1,8 MMA is regarded as a primary marker of cobalamin deficiency and there are increasing data that high homocysteine concentrations may contribute to occlusive vascular disease, cognitive dysfunction, and adverse pregnancy outcomes and malformations.7,9,10 Functional vitamin B12 deficiency in vegetarians may contribute to hyperhomocysteinemia in this population.3
Homocysteine and MMA are sensitive markers of cobalamin status and are used for the diagnosis and follow-up of cobalamin deficiency. Homocysteine is also elevated in folate deficiency and is used as an indicator of this deficiency state. MMA is a sensitive but specific marker of cobalamin function, although renal dysfunction may also cause significantly elevated MMA concentrations.9 Homocysteine is elevated in both folate and cobalamin deficiencies and also in pathologic states such as renal failure, thyroid dysfunction, coronary artery disease, and the acute phase after a cardiovascular event.7,9,10
A vitamin B12 test is used to check for megaloblastic anemia and to identify the cause of certain dementias or other nervous system symptoms (i.e., peripheral neuropathy). Vitamin B12 is usually measured at the same time as folic acid because a megaloblastic anemia may be caused by a deficiency of either vitamin. The two metabolic markers MMA and homocysteine are generally considered more sensitive indicators of vitamin B12 status than are plasma cobalamin levels.9,11 Homocysteine is an intermediary amino acid formed during the metabolism of methionine, an essential amino acid derived from protein. Hyperhomocysteinemia (> 15 µmol/L) induces vascular endothelial dysfunction and is considered to be an independent risk factor for atherosclerosis and cardiovascular disease (CVD). Treatment with folic acid, pyridoxine hydrochloride (vitamin B6), and vitamin B12 has been shown to reduce homocysteine levels in intervention studies and to reverse endothelial dysfunction independent of the effect of lowering homocysteine levels.11-14 Therefore, it is reasonable to propose that lowering homocysteine levels with folic acid and B vitamin supplements may help to decrease hyperhomocysteinemia.7,10-12
The most common screening test for vitamin B12 deficiency is the measurement of total plasma or serum
vitamin B12. Although cutoffs vary among assays and laboratories, a total vitamin B12 concentration < 148 pmol/L (< 200 pg/mL) is commonly considered indicative of vitamin B12 deficiency.1,2,5 High levels of vitamin B12 can occur in liver disease (such as cirrhosis or hepatitis) and some types of leukemia. However, the vitamin B12 test is not usually used to diagnose these conditions. Rarely, high levels may be found in obese or diabetes patients.
Causes of vitamin B12 deficiency include malabsorption, low dietary intake, strict vegetarian diet, pernicious anemia, gastric bypass or gastrectomy, ileal disease or resection, pancreatic insufficiency, absence or dysfunction of intrinsic factor, bacterial overgrowth, and impaired utilization.1,2
The most common symptoms of anemia include fatigue, shortness of breath, and palpitations. Vitamin B12 deficiency anemia may also be caused by a lack of intrinsic factor—pernicious anemia. The patient’s digestive system cannot absorb B12 properly. Signs and symptoms of pernicious anemia may include: a sore mouth and/or tongue, weight loss, pale or yellowish skin, diarrhea (sporadic), menstrual problems, greater susceptibility to infections.1,11 If the deficiency continues untreated the patient may have neurological signs and symptoms (e.g., tingling or numbness of the fingers or toes, general muscle weakness, difficulty walking, irritability, confusion, forgetfulness, tender calves).11
Who should be tested?
Pernicious anemia patients; approximately 60% have low RBC folate levels because vitamin B12 is required for normal transfer of MTHF from plasma to RBCs
Patients with elevated homocysteine
Patients post gastric bypass
Patients suspected of having macrocytic (megaloblastic) anemia; symptoms are weakness, fatigue, difficult concentration, irritability, headache, palpitations, and shortness of breath
Patients with peripheral arterial disease (PAD)
Patients with cognitive dysfunction, depression, mental changes, dementia, or insomnia
Patients with inadequate intake (e.g., malnutrition, malabsorption), increased demands (e.g., pregnancy, infancy), diseases associated with rapid cellular proliferation (hemolysis, leukemia, exfoliative dermatitis), jejunal diseases, short-bowel syndrome, and bacterial overgrowth
Patients on a strict vegetarian diet who may be deficient
Patients with chronic inflammatory bowel diseases
Patients with alcoholism, which may cause significant malnutrition and folate transport defects
Drugs (e.g., sulfasalazine, phenytoin, primidone, phenobarbital, oral contraceptives, methotrexate, triamterene) may reduce folic acid absorption and enhance folate deficiencies when patients on these drugs are not receiving supplementation
Treatment Considerations
Vitamin B12 and folate deficiencies usually require lifelong treatment with supplements. Lack of gastric intrinsic factor necessitates vitamin B12 injections. Once the diagnosis of vitamin B12 deficiency has been confirmed efficient treatment can be ensured either by injections every 2-3 months or by a daily dose of 1 mg vitamin B12.11 Patients who are taking metformin are at increased risk for vitamin B12 deficiency and may benefit from sublingual vitamin B12 supplementation.15 Vitamin B12 administration will increase red blood cell production, which may increase the need for iron supplementation as well.11
References
Snow CF: Laboratory diagnosis of vitamin B12 and folate deficiency; a guide for the primary care physician. Arch Intern Med 1999;159:1289-1298
Jordan NS: Hematology: Red and white blood cell tests. In: Traub SL, ed: Basic Skills in Interpreting Laboratory Data, 2nd ed. Bethesda, MD: American Society of Health System Pharmacists, 1996. pp. 302-304.
Herrmann W, Schorr H, Purschwitz K, et al. Total homocysteine, vitamin B12, and total antioxidant status in vegetarians. Clin Chem 2001;47(6):1094–1101.
Loikas S, Koskinen P, Irjala K, et al. Vitamin B12 deficiency in the aged: a population-based study. Age and Ageing 2007;36:177–183.
Miller JW. Assessing the association between vitamin B12 status and cognitive function in older adults. Am J Clin Nutr 2006;84:1259–60.
Ryan-Harshman M, Aldoori W. Vitamin B12 and health. Can Fam Physician 2008;54(4):536-41.
Stanger O, Herrmann W, Pietrzik K, et al. Clinical use and rational management of homocysteine, folic acid, and B vitamins in cardiovascular and thrombotic diseases. Z Kardiol 2004;93:439-453
Christen WG, Glynn RJ, Chew EY, et al. Folic acid, pyridoxine, and cyanocobalamin combination treatment and age-related macular degeneration in women. The Women’s Antioxidant and Folic Acid Cardiovascular Study. Arch Intern Med 2009;169(4):335-341.
Monsen AL, Ueland PM. Homocysteine and methylmalonic acid in diagnosis and risk assessment from infancy to adolescence. Am J Clin Nutr 2003;78:7-21.
Selhub J. The many facets of hyperhomocysteinemia: studies from the Framingham cohorts. J Nutr 2006;136:1726S-1730S.
Hvas AM, Nexo E. Diagnosis and treatment of vitamin B12 deficiency. An update. Haematologica 2006;91:1506-1512.
Homocysteine Lowering Trialists’ Collaboration. Dose-dependent effects of folic acid on blood concentrations of homocysteine: a metaanalysis of the randomized trials. Am J Clin Nutr 2005;82(4):806-812.
Moens AL, Vrints CJ, Claeys MJ et al. Mechanisms and potential therapeutic targets for folic acid in cardiovascular disease. Am J Physiol Heart Circ Physiol 2008;294:H1971-H1977.
Title LM, Cummings PM, Giddens K, et al. Effect of folic acid and antioxidant vitamins on endothelial dysfunction in patients with coronary artery disease. J Am Coll Cardiol 2000;36(3):758-65.
Moore EM, Mander AG, Ames A, et al. Increased risk of cognitive impairment in patients with diabetes is associated with metformin. Diabetes Care 2013;36(10):2981-7.
I first heard about the Ornish Diet during medical school. I was told that this diet was the only diet proven to cause regression of artery plaques and that everyone should be eating this way.
I have had a couple of patients who went on the Ornish Diet because they had heard that Dr Ornish’s diet had completely cleared the arteries of plaque.
Cardiovascular disease is the leading cause of death in the United States and my primary focus is optimal health and prevention of disease. I will implement any therapy or intervention that helps us achieve that goal.
Since I’d heard so much about the benefits of the Ornish Diet I decided to review the data myself. Here is a summary of his study.
Dean Ornish, MD demonstrated a minor reduction in artery stenosis. That means he states that he was able to increase the size of the arteries using his diet and lifestyle changes. Let’s take a look at his study.
Originally 93 patients met criteria to be included in the study and these 93 were then randomized into the control group and the experimental group. Each of these patients had coronary atherosclerosis documented by quantitative coronary arteriography. However, after randomization, only 28 of the experimental group patients agreed to participate and only 20 of the control group agreed to participate.
These patients were originally to receive a 2nd angiogram at 1 year but the study was later extended so these patients were to have a 3rd angiogram at year 5. 20 experimental patients and 15 control patients continued the study and had an angiogram at 5 years.
The experimental (intervention) group:
These patients received moderate aerobic exercise, stress management training, smoking cessation, group psychosocial support, and a 10%-fat vegetarian diet. They were instructed to avoid simple sugars and to emphasize the intake of complex carbs and other whole foods.
The control group:
These patients were told to follow the advice of their primary physician.
Coronary Artery Lesions:
Angiography was performed at baseline, 1 year, and 5 years. The Ornish Diet improved coronary artery stenosis whereas the traditional approach had an increase in stenosis.
Ornish – stenosis improved from 38.92% at baseline to 35.85% at 5 years. This is a 3.07% absolute improvement.
Traditional – stenosis worsened from 42.50% at baseline to 54.27% at 5 years. They got worse by 11.77%.
Interestingly, the Ornish group with the highest adherence had the best effect while those with the lowest adherence did halt progression of stenosis but did not have regression.
In the ‘traditional’ group they analyzed those who started lipid-lowering medications:
Lipid lowering meds – stenosis progressed from 45.7% to 51.7% (absolute difference of 6%)
No lipid lowering meds – stenosis progressed from 45.7% to 59.7% (absolute difference of 19%)
Risk Factor Changes:
Ornish –
weight – lost 23.9 lbs at 1 year but gained some back for a total loss of 12.8 lbs at 5 years
LDL – decreased from 143.8 mg/dL at baseline to 115.35 mg/dL at 5 years (28.45 mg/dL change) but the P value was 0.76 which makes this statistically insignificant.
ApoB – increased from 1.000 to 1.014
HDL – decreased from 40.05 mg/dL to 34.75 mg/dL (5.3 mg/dL change)
Triglycerides – increased from 227.8 mg/dL to 236.1 mg/dL (8.3 mg/dL change)
Blood pressure – decreased from 135/82 to 130/77
Traditional –
no significant change is weight at 1 or 5 years
LDL – decreased from 166.40 mg/dL at baseline to 133.8 mg/dL at 5 years (32.6 mg/dL change)
ApoB – decreased from 1.024 to 0.991
HDL – decreased from 52.36 mg/dL to 49.27 mg/dL (3.09 mg/dL change)
Triglycerides – decreased from 223.3 mg/dL to 211.5 mg/dL (11.8 mg/dL change)
Blood pressure – decreased from 137/80 to 123/74
Of note, the change in BMI was significantly correlated with the change in stenosis in the control group only. Those who gained weight were more likely to show progression of their atherosclerosis.
Angina:
Ornish:
Frequency (x/wk) – decreased from 5.8 to 1.6
Duration (minutes) – decreased from 3.1 to 0.9
Severity (1-7 scale) – decreased from 1.5 to 0.9
Traditional:
Frequency (x/wk) – decreased from 1.4 to 0.9
Duration (minutes) – decreased from 3.2 to 1.0
Severity (1-7 scale) – decreased from 0.6 to 0.6
It should be noted here that 5 patients in the traditional group reported increased angina and 3 of these patients underwent coronary angioplasty between years 1 and 5. In my opinion, these results should have been excluded as you are now comparing a dietary intervention with a surgical intervention and confounds the results making them uninterpretable.
Also, the P Value for all 3 measurements was statistically insignificant at 5 years. This means that all of these reductions could have occurred by chance alone.
Cardiac Events:
The number of cardiac events during the 5 year follow up:
Ornish
Myocardial infarction – 2
Angioplasty – 8*
Coronary artery bypass graft – 2
Cardiac hospitalizations – 23*
Deaths – 2
Any event – 25*
Traditional
Myocardial infarction – 4
Angioplasty – 14*
Coronary artery bypass graft – 5
Cardiac hospitalizations – 44*
Deaths – 1
Any event – 45*
*Only these events were statistically significant between groups.
I find it interesting that twice as many people died in the treatment group. Of course, this means nothing in regards to the study itself.
Discussion
There was a statistically significant difference in the primary outcome between the Ornish (experimental or treatment) group and the control group. While the Ornish intervention was beneficial when compared to the traditional medical approach we must use caution in interpreting these results. I wonder if this outcome has less to do with the benefits of the Ornish intervention or the detriment of the traditional medical approach.
One conclusion is that patients with cardiovascular atherosclerosis should be on the Ornish Diet & Intervention. However, another plausible conclusion is that no patients with atherosclerosis should be following the traditional medical approach and advice from their doctor.
This study is actually doing a head to head comparison of two different interventions. It would be interesting to see a study comparing the Ornish Diet to a group doing nothing different than the patient would normally do on their own.
There are multiple outcomes that are reported in the study: LDL, HDL, weight, blood pressure, artery stenosis, chest pain, etc. The Ornish Diet does appear to improve outcomes related to cardiovascular disease when compared to the traditional medical approach. However, a larger sample size would most likely provide more clarity.
There are several factors that confound the results of this study including limited study population and mid-study interventions such as angioplasty for worsening angina.
Clearly, we want as much improvement in the artery as possible and the Ornish Diet does seem to have benefit in this regard. However, we are more than simply arteries. Low fat diets have been shown to be detrimental for cognitive function as well as numerous other parameters. We should exercise extreme caution in recommending these low-fat diets when we are trying to optimize the overall health of our patients. While I don’t believe that a low-fat dietary approach is the best for optimal health, it does appear to be a better approach than simply following your typical doctor’s advice.
Vitamin C is a very important nutrient for a number of reasons. It is essential for several functions in the body which I’ve listed below. It is extremely safe. In fact, in the absence of kidney damage there are no known toxicities, especially if taken IV.
Good sources: Rapid growing veggies (cabbage, broccoli, asparagus, brussel sprouts), citrus fruits, and raw potatoes, organ meats (liver)
RDA: 60 mg/d. There is an active pool in the body of about 1500 mg. There is a limit to Vit C absorption. If you consume 100 mg then 100% is absorbed. However, if you consume 12,000 mg then only 16% is absorbed. However, IV Vitamin C can achieve very high serum levels without toxicity signs or symptoms.
Functions: Vitamin C is required for several metabolic functions in the body. One of its major roles is in the synthesis of collagen and elastin, the main structural proteins of skin, cartilage and blood vessels. It is also necessary in the production of several stress response hormones including adrenalin, noradrenalin, cortisol and histamine, and it is required in the synthesis of carnitine, an amino acid that facilitates the conversion of fatty acids into energy within the mitochondria. Vitamin C protects against heart disease in several ways: it helps dissolve arterial plaque, reduces free radical oxidation of cholesterol, decreases levels of the atherogenic lipoprotein Lp(a), and maintains the elasticity of vascular walls which helps control hypertension. In addition, vitamin C boosts immunity by increasing production of white blood cells, increasing levels of antibodies and interferon and modulating prostaglandin synthesis. It enhances iron absorption, promotes efficient wound healing, and detoxifies the body by binding to certain heavy metals so they can be eliminated from the body. The anti-cancer effects of vitamin C stem from its role as a potent, water-soluble antioxidant in the plasma and cytoplasm. It also protects nucleic acids (DNA) from oxidative damage and inhibits the formation of nitrosamines (carcinogenic compounds formed in the digestive tract). Additionally, it can regenerate vitamin E and works synergistically with other antioxidants such as beta-carotene and glutathione to increase their overall antioxidant effect.
Antioxidant (see oxidative damage) – The plasma ascorbate concentration in an oxidatively stressed patient (less than 45 µmol/L) measured is lower than healthy individual (61.4-80 µmol/L) according to McGregor and Biesalski (2006). Increasing plasma ascorbate level may have therapeutic effects in oxidative stress. Individuals with oxidative stress and healthy individuals have different pharmacokinetics of ascorbate
Vitamin C donates electrons in enzymatic reactions and quenches free radicals in plasma & cytoplasm
Replenishes the antioxidant Glutathione
This protects DNA from damage
Reduces free-radical oxidation of cholesterol
Involved in numerous catalyst reactions
Collagen & elastin synthesis
Vitamin C is a co-enzyme in hydroxylation reactions. If you will recall, proline and lysine are hydroxylated to form collagen.
Promotes wound healing
Increases absorption of non-heme iron
Enhances immune function
Increases production of white blood cells and interferon
Modulates prostaglandin synthesis
Decreases levels of creatine kinase after exercise
Improves blood vessel dilation
Catalyzes conversion of dopamine to norepinephrine
Necessary for the synthesis of epinephrine, norepinephrine, cortisol, & histamine
Large doses (>2 grams) have an antihistamine effect
Inhibits histamine-induced constriction of bronchial airways
Required in the synthesis of epinephrine
Regulates GABA (Gamma Amino Butyric Acid) receptors in the central nervous system (CNS)
Cofactor for carnitine synthesis
Cardiovascular protection
Metabolizes cholesterol to bile acid conversion
Dissolves arterial plaque
May decrease the atherogenic potential of Lp(a)
Lowers glycosylated hemoglobin (HbA1c), fasting and post-prandial glucose levels in diabetic patients
Required for the synthesis and metabolism of tyrosine
Aids in the detoxification of heavy metals
Inhibits the formation of nitrosamines (carcinogenic compounds) in the stomach
Partially restores thyroid function when liver detoxification ability is compromised
Deficiency alters methylation patterns in cancer cells
Enhances the effect of clomiphene, a fertility drug
Estrogen-containing contraceptives lower vitamin C levels
Increases estradiol (E2) in women on hormone replacement therapy
Lowers aromatase in the ovaries
Lowers serum uric acid levels
Catalyzes reactions that regulate oxytocin, vasopressin, and cholecystokinin
Anti-cancer effects
Slows age-related telomere shortening in human skin cells
Protects prostate against testosterone-induced tumors
Anti-cancer effects include formation of collagen to “wall off” tumors
Inhibits hyaluronidase, an enzyme that breaks down the matrix of cell walls
High Vitamin C intake can inhibit copper absorption
enhances chromium uptake
Regenerates Vitamin E. Supplementation with large amounts of either Vitamin C or Vitamin E increases the requirements of the other
Deficiencies: Deficiency symptoms include capillary fragility (due to its role in collagen formation) which often manifests clinically as bleeding/spongy gums, loose teeth, anemia, easy bruising, tender joints, muscle weakness and poor wound healing. Subclinical deficiency can also result in lowered immunity, anemia (due to vitamin C’s ability to enhance iron absorption) and fatigue (due to its role in the synthesis of carnitine and certain hormones).
Toxicity:
Vitamin C is one of the safest substance known.
Diarrhea – it you take high enough doses orally
Kidney stones (only if there is pre-existing kidney disease) – vitamin C is metabolized to oxylate which binds with calcium. They pack together to form a stone. If you increase magnesium, it binds with oxylate (instead of calcium) which is water soluble and can be eliminated.
Dependency – If you consume large quantities orally, you can become dependent on that level of vitamin C. For example, if you consume 1 gram per day and then decrease consumption to 100 mg per day, you can have some withdrawal symptoms despite the fact that your intake is above the RDA.
Rebound scurvy – along the same lines as described above but the symptoms are those of scurvy.
Vitamin D is really more of a hormone than a vitamin and it can be synthesized in the body. It is synthesized in the skin due to sunlight exposure. It is actually a group of sterols with hormone-like activities. 1,25-dihydroxycholecalciferol (Vitamin D3) is the active form.
Good sources: There are two forms of vitamin D that you can obtain in the diet. The first is ergocalciferol (vitamin D2) which is found in plants. The other form is cholecalciferol (vitamin D3) which is found in animal sources (egg yolks, organ meats, fortified milk, and cod liver oil). 7-dehydrocholesterol is an intermediate in cholesterol synthesis. The skin can convert this molecule to cholecalciferol if exposed to UV light (most important source for us). Both of the dietary sources are inactive forms and must be converted to 1,25-dihydroxycholecalciferol to be active. There is no vitamin D in the colostrum of breast milk.
Skin-derived 7-dehydrocholesterol is converted to cholecalciferol (vitamin D by ultraviolet light (most abundant source of vitamin D) – both skin/diet-derived (ergocalciferol in plants, cholecalciferol in animal products) vitamin D are hydroxylated in liver to 25-(OH)-D3 (cholecalciferol or calcidiol)g 25-(OH)-D3 undergoes second hydroxylation (la-hydroxylase) in proximal tubules to form 1,25-(OH)2-D3 (calcitriol) which binds to nuclear receptors and activates gene transcription.
PTH and hypophosphatemia enhance la-hydroxylase synthesis. Hypercalcemia, hyperphosphatemia, and calcitriol inhibit 1-a-hydroxylase: 25-(OH)-D3 is converted into an inactive metabolite called 24,25-(OH)2-D3. Remember that vitamin D that is bought over-the-counter must be reabsorbed and hydroxylated twice before it is active: it is not 1,25-(OH)2-D3
You can see the mechanism that does this in the diagram below.
DRI: 5 mg or 200 IU
Functions: Metabolize calcium and phosphorus (bone and teeth formation). In the intestine, it increases calcium and phosphorus absorption. There is a demineralization of bone if there is not enough vitamin D. In the kidneys it regulates calcium and phosphorus levels.
vitamin D receptors are located in the duodenum, osteoblasts, kidney: (1) vitamin D, like most other steroids, complexes with nuclear receptors and activates gene transcription. (2) vitamin D when causes the releases of alkaline phosphatase (hydrolyzes calcium pyrophosphate and other inhibitors of bone mineralization) from osteoblastsg mineralization (hydroxyapatite crystals- Ca5(OH)(PO4)3) of cartilage and bone
intestinal reabsorption of calcium/phosphorous: (1) helps maintain the normal serum ionized calcium concentration (2) also establishes a good solubility product for mineralization of bone
increases renal calcium reabsorption but not phosphate reabsorption
Deficiency: Ricketts (bones are soft and pliable) in children, osteomalacia (bone demineralization) in adults, poor growth, and muscle twitching.
hypocalcemia/hypophosphaternia from decreased intestinal reabsorptiong hypocalcernia stimulates PTH, which leads to increased calcium reabsorption from the kidney and decreased reabsorption of phosphate and also mobilizes calcium and phosphate from boneg serum calcium is restored to normal or near normal, while phosphate remains low.
Establishes a low calcium-phosphate solubility product – defective bone and cartilage mineralization (area of growing epiphyseal plate) in children (called rickets) and defective bone remodeling in adults, restricted to the organic matrix at thebone-osteoid interface (called osteomalacia)
Causes of vitamin D deficiency–
chronic renal failure (CRF) is the most common cause
(1) due to a lack of ω-hydroxylase
(2) unlike, non-renal causes of vitamin D deficiency, phosphorous levels are high owing to loss of phosphate excretion: 2o hyperparathyroidism can bring the phosphate levels down into normal or near normal range over time
poor diet: alcoholism, elderly
malabsorption: e.g., celiac disease
liver disease: e.g., cirrhosis: decreased first hydroxylation
drugs enhancing cytochrome P-450 system:
increases metabolism of 25-(OH)-D3
e.g., alcohol, phenytoin, barbiturates
e.g., a patient on birth control pills who is taking any of these drugs could become pregnant, since the metabolism of the hormones in the pill is increased
hypoparathyroidism/hyperphosphatemia: decreased 1-a hydroxylase synthesis
genetic diseases:
(1) 1-a-hydroxylase enzyme deficiency: type I vitamin D-dependent rickets
(2) deficiency of vitamin D receptors in target tissue: type II vitamin D-dependent rickets
Toxicity: Must be chronic to be toxic. Interestingly, toxicity is more about balance with other vitamins. For example, adequate amounts of Vitamin A & K2 protect against Vitamin D toxicity. It calcifies soft tissue which can cause aortic rupture. It can also cause kidney damage. High doses (100,000 IU for weeks to months) can cause loss of appetite, nausea, thirst, and stupor.
I frequently talk to people who believe that a vegetarian lifestyle is healthier and that animal proteins and fats should be avoided. The evidence to support these claims is weak at best and completely refuted by many sources.
The A To Z Trial was published in the Journal of the American Medical Association (JAMA) in March, 2007. This trial compared 4 diets:
The Atkins Diet – low carb, high protein, & high fat. Dr Atkins’ New Diet Revolution.
Traditional (Lifestyles, Exercise, Attitudes, Relationships, & Nutrition – LEARN) Diet – a ‘prudent’ diet that included 55% to 60% energy from carbohydrate and less than 10% energy from saturated fat, caloric . restriction, increased exercise, and behavior modification strategies. The LEARN Manual for Weight Management.
Ornish Diet – no more than 10% of energy from fat, very high carbs. Eat More, Weigh Less.
Zone Diet – 40% carbs, 30% protein, & 30% fat. Enter the Zone.
Each group followed the recommendations of their respective books (written in italics above). Basically, this study compared the effects of low-carb and low-fat and the results are self-explanatory.
311 premenopausal were randomized (by drawing names out of a hat, no joke) to the 4 different groups listed above. Each group received the same education on their specific diet by the same educator. Outcomes were measured as:
Weight loss at 12 months (primary outcome, the others listed are secondary outcomes)
Lipid profile (LDL, HDL, non-HDL, and Triglycerides)
% body fat
waist-hip ratio
fasting insulin
fasting glucose
blood pressure
So what were the outcomes? Atkins was as good as or better in every metric compared to the other diets!
Zone – decreased insulin 1.5, decreased glucose 1.6
Blood Pressure
Blood pressure winner = Atkins
Blood pressure was improved in each group. Systolic/diastolic pressure decrease is reported in mm Hg.
Atkins – 7.6/4.4
LEARN – 3.1/2.2
Ornish – 1.9/0.7
Zone – 3.3/2.1
So for those of you who fear fat, bacon, butter, lard, and meat and believe that carbs, whole grains, and avoidance of fat in your diet is the way to do, think again. The scientific evidence simply is not in favor of these beliefs.
This study was published in JAMA yet, ironically, the dietary advice of the American Medical Association is to avoid fat and eat carbs. When will they start listening to their own data?

 PREDIMED Study – Traditional Mediterranean Diet (TMD)
PREDIMED Study – Traditional Mediterranean Diet (TMD)