Outbreaks of Ebola Hemorrhagic Fever are scary! Although there isn’t a known cure for the disease there are a number of things that you can and should do to increase your health, prevent the disease, and lower your chances of death if you do get the virus.
What is the Ebola Virus?
Ebola is a virus that is believed to have started in animals and transmitted to humans. The first known cased of Ebola occurred August 26th, 1976 in Zaire (now called Democratic Republic of Congo). It appears that this gentleman contracted the virus while touring an area along the Ebola river. It is unknown how he contracted the virus. He died 2 weeks later.
Ebola is a virus belonging to the virus family Filoviridae. It is a hemorrhagic fever virus which causes patients to bleed both internally and externally.
What Does It Do?
The Ebola virus has a fairly specific target inside the human body. It primarily targets the liver, endothelial cells, and the reticuloendothelial system (i.e. Macrophages).
After a patient is exposed to the virus there is an incubation period of 2-21 days where they experience no symptoms. Even though it can take 21 days to show symptoms most patients begin to develop symptoms in 8-10 days.
Ebola causes symptoms of viral infection similar to many other viruses. These symptoms are mostly due to the inflammatory/immune system response to the virus. Chemicals like TNF-α, IL-6, and others are responsible for these symptoms.
It is important to understand that just because these symptoms are present it does not mean that you have Ebola!
Symptoms include:
Fever
Sore Throat
Muscle Aches and Pains
Headache
Shortly after these symptoms the patient will often develop nausea, vomiting, and diarrhea and then they may get a rash. The rash is often described as ‘maculopapular’.
The last set of symptoms includes liver dysfunction, kidney dysfunction, and bleeding both inside and outside of the body. These symptoms are more specific to the hemorrhagic fever viruses.
How Do You Get It & How Is It Spread?
Ebola is spread by direct contact with bodily fluids from an infected person. Body fluids that can transmit the virus include:
Blood
Saliva
Mucus
Vomit
Feces
Semen
Sweat
Tears
Urine
Breast Milk
These fluids can contain the virus. Once these fluids containing the virus particles makes contact with the nose, mouth, eyes, open wounds, cuts, or abrasions then that person can contract the virus.
It has not been established that you can get Ebola by breathing it! They have been able to create droplet in the lab that are ‘infectious as breathable’ but this has not been seen in the real world and there have been no documented cases of airborne transmission.
An Ounce of Prevention…
There are no known treatments for Ebola. Mortality Rates (meaning how many people die from it) seems to be holding fairly steady around 50% although one outbreak had a Mortality Rate of nearly 90%.
The best thing you can do is to prevent getting the virus altogether.
I like to classify prevention strategies in layers based on your risk. Healthcare workers and those people who are likely to come in contact with infected persons would require many more preventive strategies. However, the average person should employ some basic strategies based on their low risk of exposure.
Wash your hands frequently
Clean surfaces with sanitizing alcohol or bleach based solutions
Properly cook foods if they are at risk for being infected
Heat (30-60 minutes at 60 degrees Celsius, 5 minutes boiling) kills the virus
Avoid contact with infected body fluids
Avoid funeral or burial rituals that require handling the body of someone who died of Ebola
If you are at higher risk of exposure then consider the following:
Proper clothing: mask, gown, gloves, and eye protection
Isolate patients with Ebola
Avoid contact with bodies of those who have died of Ebola
Body fluids of patients who die of Ebola are still infectious. Also, semen of an infected person can still contain the virus for 7 weeks.
The first goal of prevention is to prevent getting the virus from the start. There is a second goal and that is to prevent dying of the infection. You’ll notice that the average Mortality Rate of Ebola is 50%. Survivors tend to recover fairly quickly.
While there has been no discussion about who dies from the disease and who recovers from it I suspect that there is a common thread of baseline health of the infected but surviving patients. I believe that the healthier you are in the beginning the more likely you are to survive an infection.
The foundation of health is through the ‘Healthy Trinity’
Nutrition
Exercise
3 R’s (Rest, Reduce stress, Recover from exercise)
This is our primary focus at Revolution Health & Wellness Clinic.
Treatment Options
Again, there are no specific treatments for Ebola. That means we need to focus on supportive care and consider any option that could possibly improve your chances of survival.
A number of antiviral medications are being tested and some show promise but nothing has been approved as of the time of this writing.
Clomiphene and Toremifine (Selective Estrogen Receptor Modulators) have been shown to inhibit the Ebola virus in vitro. This has not been tested in humans.
Some calcium channel blockers (CCBs) have shown to block the entry of the virus into cells (again, in vitro).
Melatonin has shown benefit in vitro.
Blood transfusions from patients who have recovered have suggested promise. The idea is that they have developed antibodies against the virus that may help fight the infection. 7 out of 8 people given the infusions in 1 study recovered though the infusions were given late in the course of infection and may have been recovering anyway.
Alternative Therapies – none have been tested in humans. However, nanoparticle silver has been shown effective in vitro. Part of the problem is that there has not been an established deliver route nor dose. Also, I would strongly advise any possible therapies that are not harmful but potentially beneficial. There are a number of alternative therapies that could be considered even though not proven effective. We offer many of these in our clinic.
Contact us today to make an appointment to optimize your health.
“How old would you be if you didn’t know how old you were?” Satchel Paige
Skin is the largest and most visible organ in the human body, our “first impression” organ. Unfortunately, our skin isn’t great about keeping secrets about our health and the impact of skin conditions can have a big impact on our well-being. When we look at common skin conditions, we are seeing premature signs of aging, areas of discoloration (hyperpigmentation), acne, scarring, dry skin, inflammation and other sensitivities. Skin vitality exemplifies functional medicine at it’s core. Having optimal function or dysfunction in one organ system impacts various other organ systems. Let’s look at 5 areas that impact the condition of our skin.
Hormones: Life’s little ups and downs.
Aging itself is not a disease but a process. What we’ve come to expect as we age is often a presentation of the symptoms of underlying hormonal changes.
Testosterone: During puberty, rising testosterone levels cause an increased production of sebum in the sebaceous glands found on hair follicles. These glands begin to clog as a result of this increased production, providing a wonderful place for bacteria to move in and get comfortable which, in turn, produces the all too familiar white-heads and black-heads.
Estrogens: Estrogen is crucial for stimulating collagen production. Collagen provides the network beneath the skin that provides the bouncy, healthy, youthful appearing skin. Estrogen levels begin to decline at a rapid rate around age 35, resulting in a drop in the production of collagen and elastin. The visible changes in skin from this decrease in collagen and elastin are thinning skin and the formation of fine lines and wrinkles. Decreasing estrogen levels also result in a loss of proteins that hold moisture in the skin, leading to dry, itchy skin.
Nutrition: Parting is such sweet sorrow
It’s common for people to associate nutrition with skin by thinking of greasy, fatty foods but when it comes to macronutrients, overconsumption of sugars have the largest impact on your skin. By sugars, we are talking not only about sweets but also any refined carbohydrates. Think bagels, pasta, donuts, cereal, crackers, pretzels, soft drinks and yes…even that glass of summertime lemonade. These processed, refined foods break down into (you guessed it) glucose, raising blood sugar levels. These glucose molecules can cross-link and attach to proteins (specifically COLLAGEN) in a process called glycation. This sticky sugar/collagen molecule is called “advanced glycation end product” or AGE’s. AGE’s break-down and degrade collagen and elastin resulting in an increase in cellular aging which looks back at us in the mirror as stiff, brittle skin.
Vitamins & Minerals: Small but fierce
In addition to considering the importance of food intake, micronutrients are essential for skin health and topical application of many vitamins and minerals have shown tremendous improvements in the quality of your skin.
Retinoids (a vitamin A derivative) cause an increase in cell turnover and new cell production resulting in more collagen. This increased cell turnover causes a reduction in brown spots and improves the texture of skin, plus it is effective for treating acne by keeping pores unclogged.
Vitamin C promotes skin health in two distinct ways. First, it is a powerful antioxidant and protects skin cells from damage caused by environmental toxins or sun exposure. Second, vitamin C stimulates the synthesis of collagen production and is crucial in the formation of the collagen protein itself.
Vitamin E is potent antioxidant that absorbs energy from UV rays protecting the skin from sun exposure. Vitamin E has been shown to have anti-inflammatory properties and aids in skin moisture, decreasing skin roughness.
Other nutrients and minerals can impact your skin. Silica is a trace mineral essential for collagen formation, Zinc has anti-inflammatory properties and decreases sebum, therefore can be an effective means of treating acne. Hyaluronic acid is a protein that binds and attracts water, producing volume and fullness. Coenzyme Q-10 enhances the regeneration of Vitamin E and assists fibroblasts in producing more collagen.
External Toxins: Under siege
Skin is unique because it functions both as a barrier and protector from the outside world but is vulnerable to damage from exposure to that outside world. The effects of UV exposure from the sun creates discolorations known as age spots. UV exposure accelerates wrinkling with damage caused by free radicals. These free radicals destroy cell membranes and break down collagen, leading to wrinkles. Protecting your skin is so important to reduce the risk of UV damage. Look for sunscreen that offers barrier protection in the form of zinc oxide over chemical protection like retinal palmitate to protect against exposure to potentially harmful chemicals.
Smoke is another external toxin know to damage skin cells and impact the appearance of your skin. Cigarette smoke accelerates the aging process by causing constriction of blood vessels which delays healing time. This impacts skin by increasing redness and the appearance of scars.
Products: Where the rubber meets the road
A 2009 study out of England reported that the average woman was applying over 500 chemicals to her body a day. You can read more about this study here.
Are all of these chemicals harmful?
There’s likely not a solid answer but the reality is that we are slathering so many products all over our bodies every day and these products do get absorbed into our bloodstream. Several products are known to be harmful or have toxic effects and others are known to be safe but how reasonable is it to know every chemical’s potential outcome?
So, what should you look for when choosing skincare products? Choose products that do not contain parabens, detergents or fragrance. Parabens are used as a preservative but have known adverse effects like hormone disruption, infertility and organ system toxicity. Products that contain detergents have a degenerative effect on cell membranes and are known irritants to skin. Fragrances often contain hormone disrupting xenoestrogens as well.
How can Revolution help?
We know that our organ systems are connected. The function or dysfunction of any part of our body will impact other organ systems. Using an integrative approach, we can work with you to identify root causes of skin problems and work together to correct them. We offer bioidentical hormone replacement therapy, Spectracell Micronutrient testing, pharmaceutical grade supplements, cutting-edge skincare products with iS Clinical and Revision Skincare, and collagen-induction therapy with SkinPen.
Call today to schedule an appointment 918-935-3636.
We see a lot of autoimmune conditions in our clinic. We also see a fair amount of other conditions that are the result of impaired immune dysfunction. Many of these issues can be very frustrating to treat. However, there is a therapy that holds great promise for a number of problems. This therapy is known as Low-Dose Naltrexone (LDN).
What is Naltrexone?
Naltrexone is a medication that was approved by the FDA in 1984. Its primary purpose is to block the opiate receptor and prevents medications such as morphine and heroine from being able to bind to those sites. The typical doses for opiate blockage is 50-150mg. Blocking these receptors also prevents some of the hormones made in your body from working. Hormones such as endorphins and enkephalins. Over the last 2 decades, these hormones have been shown to have an effect on the immune system regulation. [1, 4-6]
Why Use Low-Dose Naltrexone (LDN)?
It appears that a brief blockage of these opiate receptors between 2:00-4:00 am causes an up-regulation of vital components of the immune system by increasing these endorphins and enkephalins. Most of these chemicals are generally produced in this time window. Blocking these receptors briefly causes an increase in the endorphin and enkephalin production in the body which is the body’s way of trying to overcome the blocked receptors. Dr Bihari noted that taking this low-dose naltrexone (LDN) at bedtime led to a doubling to tripling of low levels of beta-endorphins. It is believed that this increase in endorphins and enkephalins work on cancer cell opioid receptors and may induce cell death (apoptosis). The endorphins and enkephalins also appear to increase Natural Killer (NK) cells and other healthy immune system functions against cancer. The idea is that since these endorphins and enkephalins play a role in immune function[7], increasing their levels helps to regulate the immune system which ultimately improves many immune conditions. Low-dose naltrexone (LDN) is important because higher doses will block the receptors for a longer period of time and decrease the beneficial effect. The LDN also needs to be immediate acting meaning that it can’t be in a sustained release formula or you will lose much of the effectiveness.
What conditions can be benefited with Low-Dose Naltrexone (LDN)?
LDN therapy has been used for a number of immune related medical issues. Some physicians have noted success in a variety of diseases:
Cancer
bladder
breast
carcinoid
colon & rectal
glioblastoma
liver
lung (non-small cell)
lymphocytic leukemia
lymphoma (Hodgkin’s & non-Hodgkin’s)
malignant melanoma
multiple myeloma
neuroblastoma
ovarian
pancreatic
prostate
renal cell carcinoma
throat cancer
uterine
Neurodegenerative issues
ALS (Lou Gehrig’s)
Alzheimer’s Disease
Autism spectrum disorders
Hereditary spastic paraparesis
Multiple Sclerosis
Parkinson’s Disease
Primary Lateral Sclerosis
Progressive Supranuclear Palsey
Transverse Myelitis
Autoimmune
Ankylosing Spondylitis
Behcet’s Syndrome
Celiac Disease
Chronic Fatigue Syndrome
CREST
Dermatomyositis
Dystonia
Endometriosis
Fibromyalgia
Hashimoto’s Thyroiditis
Irritable Bowel Syndrome (IBS)
Myesthenia Gravis
Nephrotic Syndrome
Pemphigoid
Primary Biliary Cirrhosis
Psoriasis
Rheumatoid Arthritis
Sarcoidosis
Scleroderma
Sjogren’s Syndrome
Stiff Person’s Syndrome
Systemic Lupus Erythematosis (SLE)
Ulcerative Colitis
Wegener’s Granulomatosis
Other Diseases
Common Colds
Emphysema
HIV/AIDS
How do I take Low-Dose Naltrexone (LDN)?
As previously stated, the majority of the benefit comes from blocking the receptors between 2-4am. Therefore, it is recommended that you take your LDN at night before bed. We generally start the LDN therapy between 1.5-4.5 mg per day. If you have Multiple Sclerosis (MS) which has led to spasticity of your muscles then it is recommended that you stay on a 3mg dose. For patient’s with Hashimoto’s thyroiditis we start at a lower dose (1.5mg per day) because the LDN may cause a decrease in the autoimmune disorder allowing the thyroid to work more efficiently. This could cause an elevation in thyroid hormones which may require an abrupt decrease in thyroid medications in order to avoid hyperthyroidism.
Don’t some people say LDN doesn’t work?
There is a lot of information about the use of low-dose naltrexone (LDN). However, there is not a wealth of randomized, placebo controlled, double-blinded studies (RCTs) which are generally the gold-standard for scientific evidence. The first dictom of medicine is Primum non nocere – First do no harm. Physicians have a responsibility to their patients. Basically, doctors work by 2 rules:
Don’t do anything that could harm your patient
Do everything you can, except things under rule #1, to help your patient
Medicine is both art and science. However, we have lost our art and tend to religiously stick to the science part. This becomes a problem when we neglect potentially helpful therapies but don’t use them because there isn’t enough evidence. Not using good interventions simply because of a lack of data is throwing the baby out with the bathwater! The best example I’ve seen of the ridiculousness of this approach was published in the British Medical Journal where the authors searched for randomized controlled trials proving the effectiveness of the use of parachutes to prevent death. The authors concluded “As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomized controlled trials. Advocates of evidence based medicine have criticized the adoption of interventions evaluated by using only observational data.”[11] Just because there is a lack of evidence supporting the use of a medication, intervention, supplement, or procedure does not mean it doesn’t work! LDN is very safe and is an FDA approved medication being used at a fraction of the dose originally approved. Additionally, there are a number of studies which show significant promise for the use of LDN is many of the conditions listed above.
Bihari B, Drury FM, Ragone VP, et al. Low Dose Naltrexone in the Treatment of Acquired Immune Deficiency Syndrome. Oral Presentation at the IV International AIDS Conference, Stockholm, Jun 1988.
At my clinic in Tulsa we do a lot of testosterone replacement therapy (TRT). Low testosterone is associated with a number of medical concerns and many of our male patients complain of fatigue and decreased performance when their testosterone levels are low.
There are a number of ways to manage ‘Low T’ including supplementing with testosterone. When we offer testosterone replacement one of the first questions many patients ask is “Well, what about prostate cancer? Doesn’t testosterone replacement cause prostate cancer?”
There is a lot of evidence suggesting that testosterone replacement therapy (TRT) does not increase risk of prostate cancer or other problems. Here, I present several studies validating this position.
How it all began…
The question of an association between higher levels of testosterone fueling prostate cancer and low levels reducing prostate cancer dates back to a study by Dr Huggins in 1941.[1] In his study, he castrated one patient and noted an improvement in prostate cancer. He also noted advancement of prostate cancer with the administration of testosterone injections.
However, “more recent data have shown no apparent increase in pCA rates in clinical trials of T supplementation in normal men or men at increased risk for pCA, no relationship of pCA risk with serum T levels in multiple longitudinal studies, and no reduced risk of pCA in men with low T. The apparent paradox in which castration causes prostate cancer to regress yet higher T fails to cause pCA to grow is resolved by a saturation model, in which maximal stimulation of pCA is reached at relatively low levels of T.”[2] In that same article, Morgentaler concludes “there is not now-nor has there ever been-a scientific basis for the belief that T causes pCA to grow.”
Hormone levels and prostate cancer
In a study published in 2008, the investigators evaluated 3886 men with a history of prostate cancer and compared them to 6438 men without prostate cancer. They measured testosterone, free testosterone, DHEA-S, androstenedione, androstenediol, estradiol, and calculated free estradiol and found no correlations between the levels of these hormones and risk of prostate cancer.[3]
Testosterone Replacement & Prostate Cancer
Gould published a review of 16 studies evaluating various testosterone formulations. He found no risk of increased prostate cancer over the baseline prevalence. Some studies went as long as 15 years.[4]
There was another study evaluating 1365 men on testosterone replacement therapy (TRT) for 20 years. These men were screened with a digital rectal exam (DRE) and prostate specific antigen (PSA) at baseline and then every 6 months. Any abnormal changes were evaluated with an ultrasound and prostate biopsy. Their conclusion was that there was no difference in PSA, free PSA, or prostate cancer compared to baseline risk. All cancers in the treatment group were localized and curative. They felt that testosterone treatment and monitoring may be safer than no treatment.[5]
13 men with testosterone deficiency and untreated prostate cancer received testosterone replacement therapy (TRT) for a median of 2.5 years. Testosterone levels increased from an average of 238 ng/dL to 664 ng/dL. There was no increase in any of the patient’s PSA nor their prostate volume during the study. 54% of follow up prostate biopsies showed no cancer. There was no local progression or metastasis.[9]
Testosterone Replacement after Radical Prostatectomy (for Prostate Cancer)
10 patients with organ confined prostate cancer had their prostates removed (radical prostatectomy). They were treated with testosterone and their PSAs were followed. After 19 months they had no detectible increase in their PSA levels (PSA <0.1) and there was no recurrence of their prostate cancer. They concluded that testosterone replacement therapy was safe in a highly select group of patients. [6]
Testosterone Replacement after Prostate Brachytherapy (for Prostate Cancer)
31 men received testosterone replacement therapy (TRT) for low testosterone after having brachytherapy. They were followed from 0.5-8.5 years (median 4.5 years). Their testosterone levels rose to 365-1373 ng/dL after starting TRT. One patient noted a transient elevation in PSA. The PSA levels were <1 in all patients. No patients stopped their TRT due to cancer recurrence or progression. The authors concluded that TRT may be used with caution and close followup after brachytherapy for prostate cancer.[7]
What does it all mean?
There does not appear to be a link to higher levels of testosterone and increased risk of prostate cancer. The proposed ‘saturation model’ appears to be an appropriate explanation for the benefit of castration explained by Huggins yet contradicted by the later studies.
Caution should be exercised when considering testosterone replacement therapy (TRT) for any patient much less in those with other risks.
A study was recently published that has the medical community in a tizzy about the risks of testosterone replacement therapy (TRT). That it may increase risk of non-fatal heart attacks.[1]
This study was a cohort study meaning that the investigators evaluated a large population of men and compared those that received testosterone replacement therapy prescriptions with those who did not and compared their risk of non-fatal heart attacks.
My intent is to discuss this topic and evaluate what this study tells us, and what is does NOT tell us, about the risks of testosterone replacement therapy. As with all studies, the results may not be as they appear in the author’s conclusions.
How the study was conducted
The investigators used the Truven Health Marketscan to collect data. This database includes diagnoses, procedures, and prescriptions. They evaluated the available data from 2006 to 2010. There was available data on enrollment history, date of birth, gender, ICD-9 diagnosis codes, treatments, and outpatient prescriptions. There was no data available on reasons for testosterone prescription, race, laboratory findings, occupational, environmental, or lifestyle factors.
The investigators then placed the patient data into cohorts provided they had at least 22 months of continuous data on the individuals. The idea was to have 12 months of data before a prescription (pre-prescription) and 90-180 days of data after a prescription (post-prescription). They compared testosterone replacement prescriptions as the treatment or test group and a PDE5 prescription (i.e. viagra) as the control group for comparison.
The testosterone prescription group included any new testosterone replacement therapy prescription that did not contain estrogen. There were 55,593 individuals in this group. They did not differentiate one form of testosterone replacement from another. There were 167,279 new PDE5 prescriptions in this timeframe. There was no data on how much medication was actually consumed in either group.
The post-prescription group was followed until one of the following occurred: they had a diagnosis of non-fatal MI, they refilled their first prescription, or 90 days after their first prescription whichever occurred first. Men with a history of MI prior to their first testosterone (or PDE5) prescription were excluded.
The Results
The authors used a pre/post-prescription ratio, what they called a rate ratio (RR), to analyze the rate of MI before and after the use of testosterone. They further broke the information down by age.
For all men: They found an increased RR of 1.36 for all men who were prescribed testosterone. Before testosterone replacement, the rate of MI among all ages was 3.48 MIs per 1000 men. After testosterone replacement, the rate for this same group was 4.75 MIs per 1000 men.
For men <65 years of age: The RR was 1.17 which was slightly increased. Before testosterone replacement, the MI rate was 3.22 per 1000 men. After testosterone replacement, the rate was 3.76 per 1000 men.
For men >65 years of age: The RR was much higher at 2.19. Before testosterone replacement, the MI rate was 5.27 per 1000 men but increased to 11.52 per 1000 men after starting testosterone replacement. It should be noted that there were only 20 MI’s in the 7,054 men > 65 years of age after starting testosterone replacement revealing relatively low numbers in an aging population.
Dicussion
This study does show an increased risk of non-fatal myocardial infarction (MI) after starting testosterone replacement therapy in men 65 yrs of age or older in the first 90 days after initiating therapy.
However, there are several issues in this study.
First, they only followed these men for 90 days. This study does not evaluate a longer-term look at the risks or benefits of testosterone therapy. It is conceivable that longer term use of testosterone lowers risk but would not be revealed in this study. Interestingly, when patients didn’t refill their testosterone prescription they followed them through to 180 days and noted a decreased risk (back to baseline) of MI in these patients. They attributed this return to baseline risk to the lack of testosterone replacement. However, they did not evaluate those that did continue to take testosterone for the same period of time. It is possible that this effect was simply due to stabilization in their physiology independent of testosterone replacement.
Next, there is no information on prescribed dose or testosterone levels. It is impossible to accurately determine the effect of testosterone replacement independent of dose. As I’ve stated before, testosterone replacement therapy (TRT) is an art and there are multiple factors that must be addressed in order to optimize each patient’s physiology. Several of these factors could increase the risk of MI if not optimally controlled. Increased estrogen levels could play a significant role but this data was unavailable in this study.
This type of data is epidemiologic. We are making observations only. The problem is that many people will read this study, take it at face value, and try to apply this across all patients who may benefit from testosterone replacement therapy (TRT).
There may be truth in this study but there are multiple potential confounding issues. I agree that further studies are needed.
Other studies show different results
There are multiple studies showing that testosterone therapy is beneficial for cardiovascular disease. Read the post on low testosterone for more information on this topic.
There is a lot of attention on testosterone these days. There are lots of Low T clinics popping up all over the place.
The issue is that low testosterone is a major health problem for both men and women. Testosterone has numerous benefits in the body. Ensuring optimal levels benefits health and performance.
Andropause is another name for Low Testosterone.
So, what are the symptoms of low testosterone and what conditions increase when testosterone is low?
Symptoms of low testosterone:
Increased heart attacks and strokes
decreased memory & intelligence
Increased dementia & alzheimer’s
Loss of drive & competitive edge
Stiffness & pain in muscles and joints
Falling levels of fitness
Decreased effectiveness of workouts
Sarcopenia
Osteoporosis
Anemia
Increased cancer
Fatigue, tiredness
Depression, mood changes, hopelessness
Irritability
Dysphoria
Reduced libido & potency: decreased desire & fantasies, decreased morning erections, decreased erectile tension, longer recovery times between orgasms, decreased intensity of orgasms
Testosterone levels tend to decline with age. However…
“We age because our hormones decline,
Our hormones don’t decline because we age.”
– Ron Rothenburg, MD
We also see:
Increased risk of diabetes & metabolic syndrome
Increased inflammation
Increased risk of cancer
Studies show that higher levels of testosterone are associated with lower mortality.
A 10 year prospective study with 11,606 men between the ages of 40 and 79 years validated this. In fact, they concluded that low testosterone predicts cardiovascular disease.[1] It should be noted that these were natural testosterone levels not levels in patients receiving testosterone replacement therapy.
In this study, men with a testosterone level above 564 (compared to 350) had a 41% lower chance of dying for any reason. Also, the risk of dying decreased 14% for every 173 point increase in testosterone. So, a testosterone level of 1000 compared to 300 had a 57% decreased risk of death.
But what about those patients who are receiving testosterone replacement therapy (TRT)? Does it lower their risk too?
A study of 1031 male veterans over the age of 40 years with a total serum testosterone level of < 250. 398 of these patients began testosterone replacement therapy. After 4 years of therapy, the mortality in the treated group was 10.3% while in the untreated group it was 20.7%. This was very statistically significant with a P of <0.0001. This means that there was less than a 0.1% chance that these findings were due to chance.[2]
Also of note in this study, prostate cancer in the testosterone replacement therapy group was 1.6% whereas it was 2.0% in the untreated group.
Higher levels of testosterone improve cognitive function
Lower testosterone levels are associated with lower cognitive function and testosterone replacement therapy improves this function.[3,4]
Testosterone Replacement Therapy (TRT) prevents the production of beta amyloid precursor proteins in men which are increased in Alzheimer’s Disease.[5,6]
In a study by Tan, 36 newly diagnosed Alzheimer’s patients had their serum testosterone levels measured. 10 of these 36 patients had a testosterone of <240. 5 of the 10 received testosterone replacement therapy (TRT) and 5 were given a placebo. The placebo group gradually deteriorated but the TRT group improved over 1 year.[7]
In patients with low testosterone, testosterone replacement therapy (TRT) is effective in improving mood when psych drugs don’t work.[8]
Testosterone Replacement Therapy increases nocturnal and spontaneous erections and improves mood.[9]
High free Testosterone levels were associated with better performance on tests of memory, executive function, and spatial ability and with a reduced risk for Alzheimer’s Disease as well as improved cerebral blood flow.[10]
Low testosterone in associated with Cardiovascular Disease Risk
The lower the testosterone and free testosterone the more likely there was CAD. Testosterone improves exercise induced ST depression. Testosterone dilates coronary arteries. Low testosterone is associated with dyslipidemia. Higher levels of endogenous testosterone are associated with a decreased risk of cardiovascular death.
Low-dose supplemental testosterone treatment in men with chronic stable angina reduces exercise-induced myocardial ischemia.[15]
Short-term administration of testosterone induces a beneficial effect on exercise-induced myocardial ischemia in men with coronary artery disease.[16]
Short-term intracoronary administration of testosterone, at physiological concentrations, induces coronary artery dilatation and increases coronary blood flow in men with established coronary artery disease.[17]
In men with CHF, 12 weeks of treatment with testosterone was safe, well tolerated, and led to significant improvements in physical capacity and symptoms.[18]
Testosterone replacement therapy improves lipid profiles and reduces inflammatory cytokines.[19]
There is an independent inverse association between levels of testosterone and aortic atherosclerosis in men.[20]
Total and free testosterone levels in men less than 45 years of age with coronary artery disease were significantly lower than those of controls. Free testosterone levels less than 17.3 pg/mL had a 3.3 times increased risk of premature coronary artery disease.[21]
There is an inverse relationship between testosterone levels and blood pressure.[22]
Low testosterone is associated with increased aging
Lower free testosterone was independently associated with frailty at baseline and follow-up.[23]
Testosterone is a major predictor of skeletal mass. There is improved strength without exercise but marked improvement with exercise.[24]
Shores MM, Moceri VM, Gruenewald DA, et al. Low testosterone is associated with decreased function and increased mortality risk: a preliminary study of men in a geriatric rehabilitation unit. J Am Geriatr Soc 2004;52:2077e81.
Shaw KT, Dowsett M, Folkerd E, et al. Endogenous testosterone and mortality due to all causes, cardiovascular disease, and cancer in men: European prospective investigation into cancer in Norfolk (EPIC-Norfolk) Prospective Population Study. Circulation 2007;116:2694e701.
Shores MM, Matsumoto AM, Sloan KL, et al. Low serum testosterone and mortality in male veterans. Arch Intern Med 2006;166:1660e5.
Laughlin GA, Barrett-Connor E, Bergstrom J. Low serum testosterone and mortality in older men. J Clin Endocrinol Metab 2008;93:68e75.
Have you noticed the number of low testosterone clinics in Tulsa, Oklahoma?
In fact, Low T centers who specialize in low testosterone and testosterone replacement therapy are springing up all over the country. If you search the internet for “Tulsa Testosterone,” “Low T Tulsa,” or some other variant of testosterone replacement therapy you will undoubtedly find a number of ‘hits.’
What is the big deal with testosterone?
Why the sudden interest?
Testosterone is a steroid hormone present in both men and women. It has very important effects for each gender but it is responsible for many of the male characteristics such as hair distribution, muscle mass, sex function and drive, and many others.
What happens if Testosterone is low?
Well, for starters, you often feel bad!
There are a number of symptoms associated with low testosterone in women and in men. I’ve written a post specifically on the problems with low testosterone in men. The following applies to men and women but these are the symptoms that most women would notice:
There are a few things to consider here. The first thing is to ask ‘why are my testosterone levels low?‘ It may be impossible to answer this question but it has to be addressed. As you probably already know, our main focus at Revolution Health & Wellness Clinic is to identify and treat the underlying medical condition cause the problem! We’ll focus on this component in a later post.
After considering the underlying issue then we can consider what else needs to be done. There are 2 options: a natural approach to try to raise testosterone levels without actually giving testosterone and testosterone replacement therapy (TRT).
Supplementing with exogenous testosterone should not be taken lightly for a number of reasons and it is very reasonable to start with a natural approach. Here is how I would approach that:
Decrease caloric intake – lower calorie intake has been shown to increase testosterone levels
Increase protein intake –
Arginine, Leucine, and Glutamine – amino acids
Exercise – you’ll want to focus on the high intensity, interval type training
Get enough sleep
Reduce stress –
Lose weight – if obese or overweight
Zinc (if deficient) – zinc is needed for the metabolism of testosterone
TestoPlex (Testosterone Revolution) – one of our supplements which has been shown to increase free testosterone
Testosterone Replacement Therapy (TRT)
You may have tried the natural approach or you’re levels may have been so low that you want to take a form of testosterone in order to increase your levels and help get you back on the right path as quickly as possible. But, like I said earlier, this is not something that should be entered lightly.
Taking exogenous testosterone replacement (testosterone from outside your body) will very likely decrease your body’s ability to produce it on its own. Your body will shut down its own testosterone producing factories because they aren’t being told to produce testosterone since you are giving it to yourself some other way.
If you shut down all of your factories then you’ll have trouble producing it again without a little help. This is definitely something we can plan for but we may not get the desired results in the long run. You may ‘rebound’ to a level lower than ideal for you and this may mean that you need to be on Testosterone Replacement Therapy (TRT) in some form long-term. This isn’t necessarily a problem but definitely something that should be considered.
Disclaimer: testosterone replacement therapy (TRT) should be reserved for patients in need of testosterone supplementation from a medical perspective. We do not prescribe, nor do we recommend any one take, testosterone replacement for performance or anabolic purposes only. While testosterone replacement therapy, under the guidance of an appropriately trained and experienced physician, is extremely safe there are potential risks that must be managed. This information is intended solely for the education of the reader in the setting of medically indicated testosterone replacement therapy.
Different Forms of Testosterone:
There are several methods for taking Testosterone Replacement Therapy (TRT). There are 4 primary methods:
Sublingual (Troches, Liquid)
Topical (transdermal) testosterone replacement – gels or creams
Injections
Pellets
Each method has its pros and cons.
Troches – these are waxy little pills that you place under your tongue and allow them to dissolve. The medicine goes directly into your bloodstream but it takes a while for the troche to dissolve. I typically recommend them twice daily in order to get good effects due to the relatively short half-life of bioidentical testosterone in them. The troches are compounded, or made, at a compounding pharmacy so they are made specifically for you.
Sublingual – the testosterone can also be put into a liquid which you would put under your tongue. This works basically the same way as the troches but it is a liquid so it doesn’t have to dissolve.
The oral/sublingual route (troches and sublingual testosterone replacement therapy) is not my preferred simply because I don’t know how much each patient is swallowing and how much is absorbing straight into their bloodstream. The body processes it differently. I believe there are better routes of administration.
Topical (transdermal) – Topical testosterone replacement therapy is available commercially or compounded. Your physician can prescribe topical testosterone using brand names like Axiron, Androgel, Testim, etc. These medications are available at most pharmacies with a prescription. However, they are very expensive and are fairly low concentration. If insurance doesn’t cover your testosterone replacement medication then you may be out several hundred dollars for a single month’s supply.
Compounded topical testosterone is an excellent option. With a prescription, the compounding pharmacy can make a testosterone gel or cream up to 15% concentration. Commercially available testosterone is typically around 1-2% concentration. Thus, we can give much higher doses in a much smaller volume.
I have not seen optimal results with the commercially available preparations due to the large volume required. I have seen some patients that had to use enough to cover both arms and across their chest, allow it to dry, and then apply it again in order to get a sufficient amount. That is a lot of testosterone gel!
We can get the same doses of testosterone is a much smaller volume and at a fraction of the cost in a compounded version. However, you do want to be careful and choose a reputable compounding pharmacy that you can trust!
Another important thing to consider with topical testosterone is that there can be transferrance. Transferrance occurs when the testosterone on your skin rubs off on someone else when there is skin to skin contact. This can happen several hours after you apply the gel or cream so you need to consider that as well.
Pellets – Another option for testosterone replacement therapy is subcutaneous pellets. Basically, these are small pellets containing testosterone which are implanted under the skin and slowly released over 3-6 months. My biggest concern with pellets is ensuring the correct dosing because once they are in you cannot remove them. If you place too many of them you will simply have to wait until they are absorbed. Most of the time this isn’t an issue with high quality pellets but it is something to consider.
I have heard of good, consistent results for 3 months after pellet placement but it becomes variable after that. Many have good results for 6 months but between 3 and 6 months it is unpredictable and variable. The other concern I have is with the cost. They are several hundred dollars and not covered by insurance. This makes it one of the most expensive options for testosterone replacement therapy. However, if you want to place them and forget about them then this may be a great option for you!
Injections – Testosterone Replacement Therapy (TRT) can also be given by injection. The other forms of testosterone replacement are bioidentical meaning that the testosterone in the medicine is the exact same structure as the testosterone that your body creates. The 1/2 life of testosterone is relatively short so you generally have to take those medicines 1-2 times per day in order to maintain appropriate levels.
Injections are a little bit different. The testosterone molecule is slightly altered by the addition of a ‘tail’ on the molecule which slows its absorption and effect in the body.
After an injection of Testosterone Cypionate 200mg your blood levels of testosterone increase roughly 3 fold. However, about 10-14 days later they return back to your baseline levels.
There are 2 other testosterone medications that we typically use: Testosterone Enanthate and Testosterone Propionate. Each of these testosterones have slightly different properties.
Testosterone Enanthate has a shorter half-life than testosterone cypionate but slightly longer than testosterone propionate. I generally dose this injection about every 4-5 days. Some patients prefer how they feel with this medication.
Testosterone Propionate has a shorter half-life than testosterone enanthate and I often prescribe it every 3-4 days.
Testosterone cypionate (depotestosterone) is commercially available meaning that you can get it at a standard pharmacy. However, testosterone enanthate and testosterone propionate may not be commercially available at all pharmacies. Therefore, we recommend obtaining them through a compounding pharmacy.
How often should you take your injections?
The majority of our patients do very well on testosterone cypionate injections and we generally recommend them once a week. If you are on testosterone replacement therapy (TRT) injections but only taking them every 2, 3, or even 4 weeks then either you or your doctor don’t understand the pharmacokinetics. Testosterone cypionate does not last that long in your system!
How you feel 10-14 days after your injection. If you start to notice a decline in your energy, performance, or any other testosterone related issue then ask yourself why you are only taking the injection every 2-4 weeks. Why would we only treat you half to a quarter of the time. Makes no sense! We want to dose and time your injections to get you the most appropriate therapy.
There are numerous other considerations when replacing testosterone. It is not as simply as just taking an appropriate amount of testosterone!
Taking supplemental testosterone can adversely affect a few things. It can alter your blood lipids (cholesterol), increase your hematocrit and make your blood thicker, increase DHT, and increase estradiol as discussed below. All of these issues need to be followed if you are on testosterone replacement therapy. However, I do not typically see these problems with normal physiologic levels (our target dose). I generally see these issues when the testosterone levels are too high.
Testosterone Replacement Therapy (TRT) is an art and you want an experienced artist. As I stated before, you want to consider the original problem causing low testosterone and that is first and foremost. Next, you have to consider the metabolism of testosterone as it converts to estrogen (estradiol) as well as Dihydrotestosterone (DHT). You want appropriate levels of those hormones as well.
Appropriate testosterone management addresses all of these issues to help you feel and perform your best within the confines of appropriate medical therapy.
As a Dive Medical Officer (DMO) in the military I’ve seen a lot of barotrauma. Barotrauma means that there is damage due to the pressure exposures of diving and the inability to ‘clear’ or equalize the pressures as you go deeper.
There are several areas that can be damaged by this pressure and the ears are a very common source. Its the same problem that many people get when they fly.
There are 5 conditions that make barotrauma possible. We use the acronym ‘MARGE’ to help remember them:
Membrane lined with blood supply
Ambient pressure change
Rigid walls
Gas filled space
Enclosed space
The pressure in the ears causes some damage which results in a level of bleeding that is generally equivalent to the amount of tissue damage and generally correlated to the pressures experienced.
After these pressures and damage there are often residual symptoms such as pain and pressure in the ear. Generally, these symptoms resolve over time if not reexposed to additional damage. So, how do you know how bad the damage is and how long to avoid diving?
The Teed classification of middle ear ‘squeeze’ or barotraumahelps us classify it:
Teed 0 – There are symptoms (pain, pressure, etc) but no visual changes in the ear
Teed 1 – There is vascular congestion of the pars flaccida, umbo, and vascular strip
Teed 2 – Vascular congestion of the entire tympanic membrane
Teed 3 – there is hemorrhage (bleeding) within the tympanic membrane
Teed 4 – there is extensive hemorrhage (bleeding) within the middle ear and the tympanic membrane (TM) may rupture.
Teed 5 – the middle ear is filled with hemorrhage (bleeding)
This picture shows what you’d see on otoscopic examination.
Treatment: depends on the severity of the damage and the Teed score. Generally, we will restrict diving until they are healed.
For a Teed 0-1 this is generally 8-72 hours
Teed 2-3 it is generally 1-8 days
Teed 4-5 may take up to 6 weeks if there is a perforation.
Other therapies include oral and topical (nasal) decongestants, pain control, and avoiding diving until its healed. I would consider antibiotics IF the tympanic membrane is ruptured.
What follows is more validation of the benefits of Prolotherapy and how you can often alleviate your pain, even in Tulsa, Oklahoma.
I have been in the Army a long time and we’ve seen lots of aches and pains. Medics are routinely instructed to give out Motrin (ibuprofen) for these pains. We give it out so frequently it is generally referred to as “Ranger Candy.”
I was an Athletic Trainer in college. We worked with a lot of athletes and athletic injuries. Standard medical dogma for sports injuries is RICE – Rest, Ice, Compression, and Elevation. The primary purpose for this is to reduce the inflammation and pain. We used a lot of ibuprofen like medications on those athletes as well.
For most of my adult life I thought that the best thing you could do for an injury was to treat it with these NSAIDs (non-steroidal anti-inflammatory drugs).
How They Work
NSAIDs (such as ibuprofen, naproxyn, diclofenac, meloxicam, celecoxib, etc) work by blocking an enzyme in the Arachidonic Acid pathway. Huh? What is that??
The Arachidonic Acid pathway is a series of chemical reactions that result in the formation of a number of chemicals that generally produce inflammation. It is generally triggered by an injury of some type. These chemicals cause fluid to leak out of the blood vessels and cause swelling, increase circulation causing reddness, cause irritation on the nerves (the pressure from the swelling also stimulates these nerves), and several other effects that are involved with the inflammatory process.
One of the enzymes is the cyclooxygenase (COX) enzyme of which there are 2 varieties: COX-1 and COX-2. Most of the NSAIDs on the market today are COX non-selective meaning that they inhibit both of these enzymes. The COX-1 enzyme produces some prostaglandins that are protective. Inhibiting this enzyme can interfere with platelet function and stomach lining protection.
In short, these medications decrease inflammation.
Why We Need Inflammation
Any idea how we actually heal after an injury?
Inflammation is the mechanism by which our body heals. When we decrease inflammation we are decreasing our healing mechanism. In fact, there are studies documenting a decrease in healing after an injury when taking these medications.
In a study published in the American Journal of Sports Medicine, 215 rats had a transection of the patellar tendon at the inferior pole and stabilized with a cerclage suture. They were then randomized to 7 groups. Each group received a different NSAID (ibuprofen, acetaminophen [not an NSAID], naproxen, piroxicam, celecoxib, valdecoxib, or control) for 14 days. At 14 days the rats were sacrificed and the tendons were loaded to failure.
The naproxyn, piroxicam, celecoxib, and valdecoxib groups all had failures of the cerclage suture. This means that they didn’t heal well. Ibuprofen and acetaminophen didn’t seem to have this effect. These results were statistically significant with a P < 0.001. Other studies have demonstrated impaired healing in tendons while taking ibuprofen.
Another study published in the Journal of Applied Physiology showed that runners did not develop the same collagen adaptation to running if they took anti-inflammatory medications.
So, taking NSAIDs (any of them!) is a Faustian bargain. You trade the long term decreased healing for short term pain management. You are making a deal with the devil and he will come back later to collect!
If you want to heal then you should avoid all of these anti-inflammatory medications after an injury. In fact, the only time I typically prescribe them is for non musculoskeletal pain. It simply isn’t worth it!
When you have these injuries you want your body to heal! Most things will heal themselves, on their own within about 6 weeks. However, for those injuries and pains that don’t resolve, look at prolotherapy! It helps your body heal.
It is fairly obvious that taking these medications slows or prevents the healing process. That is certainly one of the reasons that they medicines should be avoided for musculoskeletal pain. But there are other reasons as well.
Side Effects
NSAIDs inhibit the formation of prostaglandins which increase inflammation but some of them are protective as well. Some of these chemicals are protective to the lining of the stomach. Taking NSAIDs erodes this lining and makes the stomach more likely to have ulcers. They can increase the risk of gastrointestinal bleeding. For some people this can be life threatening.
The prostaglandins have a role is regulating blood flow to the kidneys. NSAIDs can affect his blood flow. This can affect blood pressure. Thus, these medications can worsen hypertension.
The thromboxanes affect the platelets. NSAIDs affect the thromboxanes altering the way platelets clump together. The platelet effect is proposed to be one of the reasons that these medications can increase the risk of cardiovascular disease. In fact, if you are having a heart attack, one of the first things we do is to stop your NSAIDs.
These effects can be profound and severe is some cases. Use of these medications is not completely benign and there are potentially severe consequences. As with everything in medicine, the risks and benefits need to be carefully weighed. In many cases, the risks of NSAIDs outweigh the benefits.
Some people may think that estrogen metabolism is a boring topic and I suppose it is. However, appropriately managing hormones as well as minimizing risk for breast cancer (and other cancers) requires an understanding of this stuff.
I previously discussed human estrogens and touched on synthetic estrogens. Part of the problem with synthetic and equine estrogens is that they tend to be metabolized differently. Hopefully, I’ll be able to convey some of the issues involved with this stuff.
Estrogens are metabolized in 2 phases: Phase 1 (hydroxylation) and Phase 2 (methylation) detoxification.
Additionally, there are 3 different pathways by which the detoxification can occur. We’ll start with the optimal pathway.
2-Hydroxy
Estradiol and estrone both go through the same metabolic pathways. The ‘2’ pathway is optimal as it has the lowest risk for cancers and other problems.
You’ll notice from the pathway above that Estrone is converted to 2-Hydroxyestrone (step 1 in the diagram). This is Phase I detoxification also known as hydroxylation.
Step 2 in the diagram depicts Phase 2 detoxification which is also known as methylation. This step takes a more toxic substance and alters it to prepare it for elimination. If methylation is not working well then we can have elevated levels of 2-OHE1 (and 2-OHE2).
2-OHE1 (2-hydroxyestrone) is considered a ‘good estrogen’ and it does not stimulate cell growth. It can block the action of stronger, potentially carcinogenic estrogens. When it is methylated to 2-MeE1 it is cancer protective. Measuring the 2-OHE1:2-MeE1 ratio is a good indicator of the body’s ability to methylate. Interestingly, low 2:16 ratio is also associated with an increased rate of developing lupus.
Moderate exercise, high-protein diets, and the supplements listed below have all been shown to raise 2-OHE1 levels.
16-Hydroxy
Another potential pathway through which estrogen is metabolized is the ’16’ pathway. This pathway, while needed, is not as desirable as the 2-Hydroxyestrone pathway.
Step 1 in the 16-Hydroxyestrone pathway is the same. It is a hydroxylation, Phase I detox. However, Phase 2 is a reduction phase and produces Estriol. Recall that estriol (E3) is a very weak estrogen.
16-OHE1 has significant estrogenic activity and studies show it may be associated with an increased risk of breast cancer. Higher levels are associated with obesity, hypothyroidism, pesticide toxicity (organochlorines), too much Omega-6 fatty acids, and inflammatory cytokines.
4-Hydroxy
The 3rd possible metabolism pathway is the 4-Hydroxyestrone pathway. This pathway is the most problematic and we want to limit estrogen metabolism through the 4-OH pathway as much as possible.
Here we have estrone being hydroxylated through Phase 1 detox and forming 4-OHE1. Step 2 is methylation of 4-OHE1 to form 4-MeE1. When 4-OHE1 is properly methylated to 4-MeE1 it is relatively benign as the 4-MeE1 is easily eliminated and risks are low.
The problem starts when methylation is inadequate as there begins to be a buildup of 4-OHE1. 4-OHE1 can then be converted to 3,4-Quinones which are pro-carcinogenic meaning that they cause cancer. That is bad news!
4-OHE1 may directly damage DNA and cause mutations which enhances cancer development. Equine estrogens increase estrogen metabolism into 4-OHE1. Women with uterine fibroids may have increased levels of 4-OHE1.
Antioxidant support is a great idea to try to limit these nasty chemicals. Consider supplements such as:
Fortunately, we are able measure each of these hormones in our patients. We can measure the individual estrogens as well as the hydroxy and methoxy metabolites. We can, therefore, better assess our patient’s risks for developing cancer and having other issues associated with poor estrogen metabolism.
We test these hormones through a urine test. We can also check homocysteine levels and we assess MTHFR status as well. These can also help guide us in the appropriate management of hormone metabolism.
How To Improve Estrogen Metabolism
We’ve determined that there are healthy estrogen metabolism pathways and less healthy pathways. So, what can we do about it?
There are a variety of substances that influence the way your estrogens are metabolized. Some are toxins that increase the unhealthy estrogen metabolic pathways and supplements and foods that induce more healthy estrogen metabolism pathways. This applies to men and women as the pathways are the same for both.
Toxins:
Xenoestrogens – natural or synthetic chemical compounds with estrogenic activity. Chemicals such as polychlorinated biphenyls (PCBs), bisphenol A (BPA), and phthalates are xenoestrogens. These chemicals disrupt normal estrogenic balance. You want to eliminate these chemicals from your environment. You may also consider a supplement which helps eliminate these chemicals from your body. Read more about this anti-xenoestrogen supplement here. Oh, and don’t forget about the hormones in a lot of the meat we tend to eat. Yet another reason to get natural, hormone free, or organic meats.
Equine Estrogens – tend to favor the 4-OHE1 pathway. Combine them with a methylation deficiency and you have a potential problem.
Good Stuff:
Diindolylmethane (DIM) – a metabolite of indole-3-carbinol (I3C). DIM increases the 2-hydroxylation of estrogens favoring the more healthy metabolic pathway. Read more about DIM as a supplement here. The goal dose is 200-300mg per day.
Flax – you want the whole flax seed, not just the oil. It is the lignans in flax that help with estrogen metabolism.
Kudzu – this herb has some phytoestrogenic effects.
Sulfuraphane Glucosinolate (SGS) – supports Phase 2 detox as well as decreases the formation of 3,4-quinones. Read more about sulfuraphane here.
Hormone Protect is one of our supplements that contains both sulfuraphane glucosinolate (SGS) and Diindolylmethane (DIM).
The human body makes 3 different estrogens and all 3 are important to optimal health. Estrogens are hormones. Hormones are chemicals that result in a cellular change when they bind to their receptors which are often in distant tissues. They are a way that the body communicates with itself.
Estrogen Receptors
Estrogens are hormones that bind to estrogen receptors. There are 2 different estrogen receptors known as α and β. There are different concentrations of these receptors in different tissues and activation of these receptors results in different results.
α estrogen receptors are primarily found in the endometrium in the uterus, breast cancer cells, and hypothalamus. Males have these α estrogen receptors in the efferent ducts of the testis. Stimulation of the α estrogen receptor (ERα) stimulates cell growth.
β estrogen receptors are found in the brain, bone, lungs, heart, kidney, prostate, intestinal mucosa, endothelial cells and ovarian granulosa cells. Stimulation of the β estrogen receptor (ERβ) decreases cell growth.
The 3 different estrogens bind to the different estrogen receptors with different affinities. Basically, each ‘likes’ the different receptors differently. These different receptors allow for different responses in different tissues.
Estrone
The first estrogen is estrone, also known as E1. It is called E1 due to the fact that it has only one hydroxyl group. Estrone commonly converts back and forth to estradiol via the enzyme 17β Hydroxysteroid Dehydrogenase (17β HSD).
Estrone preferentially (80%) binds to the α estrogen receptor (ERα). It is the predominant hormone during menopause. Many researchers believe that high levels of estrone increase a woman’s risk of breast cancer.
Estradiol
Estradiol is also known as E2 due to it having 2 hydroxyl groups in its structure. Estradiol is produced by aromatization (via the aromatase enzyme) from testosterone or by conversion via 17β HSD from estrone as described above.
Estradiol is the most potent estrogen. It is approximately 10 times more estrogenic than estrone and 80 times more than estriol. It binds equally to the α and the β estrogen receptors.
Some of the benefits of estradiol include: increases HDL, decreases LDL & total cholesterol, decreases triglycerides, helps maintain bone structure, increases seratonin, decreases fatigue, antioxidant, improves memory, helps absorption of calcium, magnesium, and zinc
Estriol
Estriol is also known as E3 due to the presence of a 3rd hydroxyl group. It is produced by conversion of estrone through the 16 hydroxy pathway. In other words, 16-methoxy estrone is the same thing as estriol. We’ll further discuss these pathways in another post. It is the predominant estrogen during pregnancy.
Estriol binds primarily (80%) to the β estrogen receptor. It is 80 times weaker than estradiol making it a weak estrogen. It can decrease LDL and increase HDL. It can also help control menopause symptoms. It helps reduce pathogenic bacteria and helps the GI tract maintain a favorable environment for the growth of lactobacilli. It also helps restore the proper pH of the vagina, which prevents urinary tract infections.
There is considerable evidence showing that estriol has a protective effect against breast cancer. Experimentally, estriol is being used in breast cancer patients. There is some controversy about this topic and understanding cancer initiation and cancer promotion explains the disparity.
These are the 3 estrogens that are produced in the human body. After menopause, estradiol production declines dramatically and can result in a number of issues including hot flashes, osteoporosis, and numerous others.
If there is a hormone deficiency that requires supplementing with hormones then we should use bioidentical hormones. We should be using the same hormones as produced in the human body. Why would we consider anything else?
Premarin was the first commercially available estrogen replacement. Premarin stands for PREgnant MARe’s UrINe. It is so named due to the fact that it is derived from the urine of pregnant horses. It is composed of estrone sulfate (50%), equillin sulfate (15-25%), and equilenin sulfate (25-35%). These hormones are often collectively called ‘conjugated equine estrogens’ (CEE). Note that none of these hormones are of the same structure as the estrogens in the human body.
Bioidentical hormone therapy uses estrogens of the exact same structure as those produced in the human body making the ‘bioidentical’. When considering hormone replacement therapy (HRT) there are a number of issues that need to be considered such as the hormones themselves, route of administration, and the metabolism of the hormones.
Optimizing health when using hormone replacement therapy addresses each of these issues and we’ll discuss more of these components in other posts.
Have you noticed that thyroid, prostate and breast cancer are on the rise? It seems like cancer in general has become a bigger and bigger problem for lots of people.
We see TONS of thyroid problems in our clinic. Traditional medical training doesn’t offer any solutions for Hashimoto’s Thyroiditis or Grave’s Disease other than thyroid ablation and thyroid hormone replacement.
Hopefully, we’ll show you why some of these thyroid issues occur and there actually is something that can be done about much of them.
This post will be an introduction to iodine and we’ll follow with information about how iodine specifically affects things like breast & prostate cancer and thyroid disease in additional posts.
Iodine is a halide. Halides are a class of chemicals on the periodic table (group VIIa) and includes Fluorine, Bromine, Iodine, Chlorine, and Astatine. Each of these chemicals are structurally similar and they can compete with each other for binding sites in the body. This gets into why these other chemicals can be detrimental to your health.
We generally get our iodine from our food but most people in the US are deficient in iodine intake. The Recommended Daily Allowance (RDA) is 150 mcg per day for your average adult but this increases during pregnancy and lactation (breast feeding). But, remember that the RDA levels are based on preventing certain diseases, and in this case it is goiter.
While 150mcg per day is sufficient for preventing goiter it is woefully inadequate for optimal health!
Numerous conditions have been associated with iodine deficiency. Here is a partial list
Mental retardation
Goiter
Increased child & infant mortality
Infertility
Breast cancer – Causes estrogen production to increase, increased estrogen sensitivity in the breast
Prostate cancer
Fibrocystic breast disease –
Cretenism
Spontaneous abortions
ADHD
SIDS
Multiple Sclerosis
One question I had was “why are so many people deficient in iodine?” There are actually a couple of reasons for this.
Inadequate iodine intake
The World Health Organization recommends taking iodized salt to enhance iodine intake. Part of the problem with this is that iodized salt consists of processed salt, stripped from its other nutrients, and iodine. Processed salt is not the best way to go for multiple reasons. However, it does increase your iodine intake.
The other problem with this is that salt has been vilified in the medical community due to its potential impact on health. Primarily in those with hypertension, edema, or congestive heart failure (CHF). These patients are often put on a low sodium diet which is also restricting their iodine intake. Many people choose to go on a low sodium diet on their own and yet others choose to avoid processed, iodized salt and use natural forms of salt instead. I can’t disagree with that.
You can also get iodine from your natural food.
Seafood tends to be higher in iodine and seaweed has a special ability to concentrate iodine making it an excellent source. Other seafood such as cod, sea bass, haddock, and perch also have higher levels.
Other foods may have some iodine as well but it really depends on the region in which the food is grown. For example, the mid-western United States tends to have lower levels.
The iodized salt mentioned above provides 77 mcg of iodine per gram of salt. This is 100 parts per million (ppm) of Potassium Iodine (KI). In order to meet the RDA (which is too low) you’d need to ingest at least 2 grams per day of iodized salt. Some sources say that you should limit your sodium intake to less than 1500mg per day. Salt is about 40% sodium which makes your total limit for salt around 5 grams per day.
Iodine Replacement
You can eat food higher in iodine as stated above. Or you can supplement with iodine. There are several forms of iodine for replacement:
Iodine
Iodide
Lugol’s Solution – 2 drops contains 12.5mg of iodine & iodide. There is 5% iodine in every 2 drops and 7.5mg (10%) of potassium iodine.
Iodoral is a tablet form of Lugol’s
Toxic loads of the other halides
I previously mentioned that iodine is a halide and these halides compete with one another for binding sites. Higher levels of chlorine, fluorine, and bromine compete with iodine and increase the need for higher levels of iodine.
Fluorine and Bromine have no redeeming value in the human body. Some would argue that fluorine is beneficial for reducing the risk of dental caries but there are some suggestions that the benefits are dramatically overrated. Additionally, the number one cause of tooth decay is sugar. We shouldn’t consume a toxic substance in order to cover up the detriments of our poor nutritional choices. Bromide has no benefit in the body and has been shown to be toxic as well. In my opinion, we should be avoiding ingesting both of these substances altogether.
Iodine Toxicity
If you look into iodine supplementation you’ll see a lot of information on iodine toxicity for sure. There is also a lot of information out there suggesting supplementing with higher than recommended doses.
It is important to remember that the tolerance to iodine intake is highly variable from person to person. Some people can tolerate higher levels than others. However, 1mg per day seems to be safe for most people without adverse effects.[1]
Some patients may require higher doses of iodine in order to optimize their health. These patients may be at higher risk for adverse events but these can be monitored. Thyroiditis, hypothyroid, and hyperthyroid are some of the more common manifestations of too much iodine intake and these can be monitored and treated should they arise.
I’ve talked about he importance of iodine for thyroid and other issues. It is important to make sure that you are getting enough.
The RDA, Recommended Daily Allowance, is based on the amount of iodine required to prevent goiter. In fact, the RDA for most nutritional issues is based on preventing a disease. It is never based on optimal levels. The RDA has set the minimum level of intake at 150 mcg per day.
Regardless of the recommended intake, most people are deficient. Do you know if you are getting enough for optimal health?
A Urine Iodine Load Test is an excellent way of making sure your levels are optimal.
There are several labs that perform this test and we’d be happy to help you get this done. Costs vary from $75-150 depending on the lab.
You can pick up this kit in our clinic and you’ll pay for it when you pick it up.
Instructions:
When you wake up, first thing in the morning, empty your bladder and flush the toilet
Take your iodine medication as prescribed
Collect all of your urine for the next 24 hours into the supplied container. When you wake up the following morning be sure to empty your bladder again and collect that specimen as well.
Interpreting The Results
Your body tends to eliminate most of the iodine you ingest. However, if you are deficient in iodine your body will tend to absorb higher quantities and eliminate less. You should eliminate 90% of the iodine you ingest. Thus, you should eliminate 45mg of the 50mg that you take at the beginning of the test. Anything less than 90% or 45mg indicates iodine deficiency.
We generally recommend replacing iodine based on your results.
Thyroid hormones are the gas pedals for your metabolism.
The thyroid gland lives in your neck. Its main job is to produce and release thyroid hormones. The 2 primary thyroid hormones are T3 & T4.
Thyroid Hormone Composition
These 2 hormones are basically composed of 2 tyrosine molecules (an amino acid) linked together and then iodine is attached to them. We can’t make these hormones without iodine.
T4, or thyroxine, has 4 iodine molecules. It is the primary hormone produced in the thyroid gland.
T3 (only has 3 iodine molecules attached), triiodothyronine, is the primary functional hormone inside the cell. It is what is responsible for most of the thyroid hormone effects.
T4 has to be deiodinated meaning that one iodine molecule has to be removed which makes T3. There are enzymes that perform this function and they are called deiodinases.
So, your thyroid gland is responsible for making these hormones. We get iodine (and iodide) from our diet as mentioned in the previous iodine post and iodine can be ingested as either iodine or iodide. Your thyroid gland tends to absorb iodide.
Iodine is an electroneutral substance meaning that it has an even number of electrons and protons so it has no charge. Iodide, on the other hand, has an extra electron making it a negative charge.
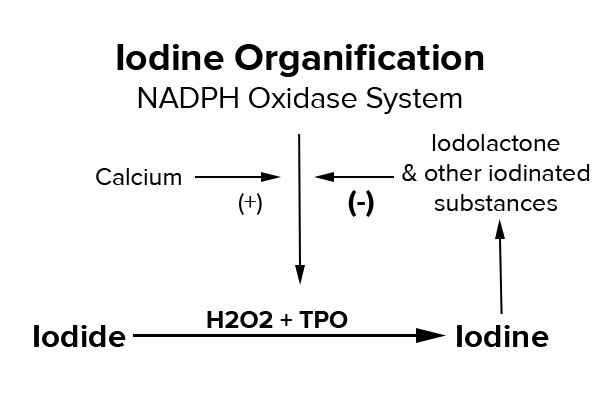
The next step in preparing iodine for incorporation into thyroid hormone is a process called oxidation. We have to prepare the iodide molecule to be utilized so it has to be oxidized. It has to convert from iodide to iodine. It does this by removing the extra electron. The thyroid gland does this through H2O2 (hydrogen peroxide) and an enzyme known as Thyroid Peroxidase (TPO).
H2O2 (hydrogen peroxide) causes oxidation. As you probably already know, excessive oxidation causes damage. Hydrogen peroxide, left unchecked, causes oxidative damage. Anything that increases the activity of hydrogen peroxide can increase the amount of oxidative damage it does.
Low Iodine Levels Lead To Autoimmune Thyroiditis (Hashimoto’s & Graves)
You’ll notice from the diagram above that when Iodine is produced, as well as δ-iodolactone and other iodinated substances, it decreases the activity of the NADPH Oxidase System. This is called product inhibition and is an important physiological control mechanism. The more iodine and iodinated substances we make the less we need so this makes sense.
However, when we have insufficient intake of iodide we cannot slow down the oxidation system because we don’t have enough iodine and iodinated substances. Are you following me so far?
Therefore, there is increased activity of H2O2 which leads to increased oxidative damage. At least some of this damage is on the thyroid peroxidase (TPO) enzyme itself. The damaged TPO is recognized by the body as foreign and potentially damaging and your body tries to fix it by developing antibodies against it. These are called Anti-thyroid peroxidase, or anti-TPO, antibodies. Elevated thyroid antibodies correspond with Hashimoto’s disease. These antibodies slowly destroy the thyroid gland.
The Importance of Antioxidants
I mentioned the oxidative damage that can damage TPO when left unchecked. Fortunately, we have a system to keep it in check. This system is called Glutathione Peroxidase and it is capable of protecting our bodies from the excess oxidative damage.
So, optimal health requires proper glutathione peroxidase function to protect from excess oxidation as well as optimal levels of iodine intake to ensure appropriate levels of iodinated substances.
Get Your Iodine Level Checked
I agree that you CAN get too much iodine but the fact of the matter is that we just don’t see it. The RDA for iodine is 150 mcg per day. This level is based solely on the amount of iodine required in order to prevent the formation of goiter. This amount is appropriate if your only goal is to prevent goiter.
We want more for our patients. We want optimal health, ideal thyroid function and the lowest risk of cancer. You need more than the RDA in order to accomplish this goal.
How do you know if you are getting enough?
Get tested. We recommend a urine test to evaluate your levels. An Iodine Load Testseems to be the best way to accurately assess your iodine levels. . This is where you take 50mg of an iodine supplement and you collect your urine for 6 hours. We then determine how much iodine you eliminate and how much you absorb. If you absorb too much then you are considered Iodine deficient and we recommend replacement accordingly.
When it comes to nutrition, athletes tend to focus on the main things…fats, carbohydrates and protein. These macronutrients are vital for nerve function, energy and muscle rebuilding but it is important to not overlook the micronutrients that your body requires to for optimal function.
Revolution Health & Wellness offers micronutrient testing through SpectraCell Laboratories. This test measures 33 vitamins, minerals, and antioxidants in your white blood cells, giving a picture of nutritional status over the last 4-8 months and evaluating your body’s ability to absorb and utilize each nutrient.
Knowing your individual nutritional status can aid with:
balancing micronutrients
muscle recovery
improving cellular energy production
reducing the risk of oxidative stress
improving immunity
regulating hormones
Micronutrient testing takes the guessing out of supplementation.
Find out what your specific, individual deficiencies are make informed choices about correcting imbalances.
Cardiovascular disease is the leading cause of death in the United States. Billions of dollars are spent studying this disease, testing for it, and trying to prevent it. Most people want to prevent having a heart attack. Just look at the amount of money spent on cholesterol medicine alone in the hopes that it will lower the risk of cardiovascular disease.
Most doctors are using the Framingham Risk Calculator which tries to predict the risk of having a heart attack based on factors such as age, gender, and cholesterol. I believe there is a better way.
A simple blood test is a strong predictor of risk for heart attacks. A 2012 study published in the Journal of Clinical Chemistry shows that elevated levels of high-sensitivity cardiac Troponin I (hs-cTnI) may predict risk of cardiovascular death.
Heart attacks occur when the blood supply to the heart is disrupted. This lack of blood supply results in a lack of oxygen (ischemia) to the heart muscle and results in damage to it. Cardiac Troponin I is a protein which is specific to heart muscle. When heart muscle is damaged it releases this protein into the blood and can be measured.
We have been using this test for over a decade in the ER to better assess if someone is having a heart attack. However, the values being measured in the ER are set to detect damage to the heart muscle in response to a heart attack. The cut off is set in the range of 100 pg/mL. Anything above that is suggestive of heart muscle damage.
Prevent heart attacks
But the interesting thing is that some studies are showing good predictive ability of Troponin I when is is elevated on a much lower level. If we can determine minute elevations of this protein then we may be able to predict a future heart attack. That would be great information!
Revolution Health & Wellness Clinic is all about preventing heart attacks. We do everything we can to identify patients at risk and intervene as early as possible. We perform the high-sensitivity Troponin I test (offered through Singulex) on our patients who may be at increased risk.
This test can help determine risk for cardiovascular disease according to the study mentioned above published in the Journal of Clinical Chemistry. In fact, if this test is elevated then you are 8.5 times more likely to die of a heart attack. That is an 850% increased risk!
Clearly we want to do everything we can to identify patients at high risk and intervene appropriately to prevent these heart attacks. hs-TnI should be incorporated into your annual blood tests and other studies to evaluate your overall risk of cardiac disease.
I try to stay out of the politics scene even though I have fairly strong political views but I feel that I simply have to comment on this because it has the potential to affect nearly everyone concerned about their health and health insurance.
There has been a lot of coverage lately about failures with the rollout of stages of ‘Obamacare’ and numerous people losing their coverage. The President felt that he needed to apologize for the way things are going. Bill Clinton has even chimed in and stated “I personally believe, even if it takes a change in the law, the president should honor the commitment the federal government made to those people and let them keep what they got” in a recent interview.
Well, here’s the real deal…
Obamacare simply cannot work with the promises that have been made. The fallout from trying to cover everyone regardless of pre-existing medical conditions is simply going to make costs go up in regards to the prices of your insurance plan. Dave Ramsey did an excellent job of describing the details in a recent video.
I don’t care if you are Democrat or Republican or TeaParty or Libertarian. This law will not work and costs are going to go up!
Insurance is a business and they are in business to make money. The idea is that their consumers pay into the ‘pool’ and if they have something go wrong and need to call on their insurance plan then the money comes from the pool. Insurance companies use actuary tables to determine the risk that each customer will need to call on these resources. The higher the risk the higher your insurance premiums. That is how the insurance game works.
Now, part of the Affordable (ironic, right?) Care Act (aka Obamacare) mandates that insurance companies cannot use these actuary tables to charge higher premiums to those at higher risk. In this case it is their customers with pre-existing conditions. Yes, these customers are much more likely to withdraw money from the pool. Therefore, the insurance companies have to increase the size of the pool in order to stay in business.
Any idea what that means?
Thats right… everyone has to pay more!
So now we have a young, healthy male that doesn’t smoke and has a very low risk of needing to file claims on his health insurance yet is having to pay much higher rates to subsidize the other, sicker people in the insurance pool.
True, there has always been an element of this but they used to be able to adjust the premiums reducing the burden on the healthier based on risk (actuary tables) but this is no longer the case.
There are obviously multiple issues with this but it is basically a communistic approach to mandated health insurance. Again, I’m not trying to be political and I’m certainly not advocating for or against President Obama but the very basis of this law is going to increase costs to most people across the board.
Granted, there absolutely needs to be health care reform as I totally agree that the system is utterly broken. But there are much better solutions out there. The law does do some good things but dramatic changes need to be made.
The topic of methylation is common in the Functional Medicine community. But what is methylation?
Simply put, methylation is a chemical reaction that occurs in every cell and tissue in your body.
Chemically speaking, methylation is the process of adding methyl groups to a molecule. A ‘methyl group’ is a chemical structure made of one carbon and three hydrogen atoms. Since methyl groups are chemically inert, adding them to a protein (the process of methylation) changes how that protein reacts to other substances in the body, thus affecting how that protein behaves. Enzymes, hormones, and even genes are proteins and the process of methylation affects them all.
Detoxification
In some instances, methylation of proteins helps the body detoxify. For example, the methylation process helps convert the toxic amino acid (homocysteine) into a beneficial amino acid (methionine). If your body cannot methylate properly, toxins build up in your bloodstream and will eventually cause disease.
Gene Expression & Enzymatic Activity
Another role of methylation is to help the enzymes in our bodies work efficiently. Enzymes are proteins that act like switches for chemical reactions – they initiate very important processes in every cell and tissue. In a similar way, methylation affects our genes, which are also made up of proteins. In fact, methylation can turn genes on or off, which can be good or bad for our health, depending on the gene.
Some nutrients affect the process of methylation quite dramatically – methyl donors (nutrients like folate and choline) actually donate methyl groups to proteins and methylating factors (nutrients like vitamin B12 and zinc) helps this process along by monitoring specific methylation reactions. How well your body methylates is important to your overall health.
What health issues can arise from impaired methylation?
As you continue to read, you will learn that disruptions in methylation processes can cause a variety of issues, including:
Heart Attack
Stroke
Dementia
Depression
Migraines
Autism
Fertility
Cancer
Birth defects
many more
What is MTHFR and how is it related to methylation?
MTHFR (methyletetrahydrofolate reductase) is an enzyme that converts folate into a usable form that our bodies need. It is a key enzyme in an important detoxification reaction in the body – one that converts homocysteine (toxic) to methionine (benign). If the enzyme is impaired, this detoxification reaction is impaired, leading to high homocysteine blood levels. Homocysteine is abrasive to blood vessels, essentially scratching them, leaving damage that causes heart attacks, stroke, dementia, and a host of other problems.
MTHFR converts 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate. It is the 5-methyltetrahydrofolate that converts homocysteine to methionine by the enzyme methionine synthase. Homocysteine can also be converted to methionine by betaine-homocysteine methyltransferase. This enzyme does not require folic acid.
Additionally, when the enzyme MTHFR is impaired, other methylation reactions are compromised. Some of these methylation reactions affect neurotransmitters, which is why impaired MTHFR activity is linked with depression. Inefficiency of the MTHFR enzyme is also linked to migraines, autism, fertility, cancer, and birth defects, all of which depend on proper methylation.
What is the MTHFR Gene?
The MTHFR gene encodes for the MTHFR enzyme. There are variations in the gene that affect the function of the enzyme. This is explained in further detail below. A simple blood test can tell you if you have a variant copy of this gene.
If I have variant copies of the MTHFR gene, what can I do?
If the MTHFR enzyme is inefficient, you may be able to compensate for your body’s inability to methylate efficiently since this biological process is dependent on several B vitamins. You may simply need more B vitamins than someone without a variant copy of this gene, such as vitamin B6, B12 (methylcobalamin) and the active form of folate (5-methyl tetrahydrofolate). Other methyl donors such as SAMe and trimethylglycine (TMG) may also provide benefits. If you have a defective copy of the MTHFR gene, it is important for you to monitor your homocysteine level as well. Fortunately, lowering homocysteine can often be done with the nutrient supplements listed above.
Determining what copies of the MTHFR gene you have gives you the ability to compensate accordingly. The old paradigm that we are simply at the mercy of our genes is now challenged. Genetic testing empowers you to take control, launching you into a new age of truly individualized healthcare.
There are DNA sequence variants of MTHFR and the two most commonly evaluated are 677 & 1298. These two differ by one nucleotide at either of 2 locations. The 677 refers to the nucleotide at the 677 position and 1298 is the nucleotide position of the other abnormality. This difference is often referred to as a Single Nucleotide Polymorphism (SNP). Abnormal variants are considered ‘thermolabile’ meaning that they measure the amount of enzyme activity after the enzyme is inactivated by heat.
The 677 MTHFR Mutation
The 677 variant of MTHFR has 2 possibilities: Cysteine (C) and Thymine (T). There are 3 different options for expression of this gene:
C/C – “normal” or “wildtype”. About 45% of the population have this genotype.
C/T – called ‘heterozygous’ and are considered essentially normal since the normal MTHFR will be able to compensate for the thermolabile MTHFR and there doesn’t appear to be any increased risk. About 45% of the population have this one.
T/T – considered to have mild MTHFR deficiency. About 10% of the population
The 1298 MTHFR Mutation
There are 2 possibilities for the nucleotide at the 1298 position, A & C. ‘A’ encodes for the normal glutamine amino acid and ‘C’ substitutes an Alanine amino acid. The C variant does not appear to affect the MTHFR activity nor homocysteine levels.
Severe MTHFR deficiency is rare and results from mutations causing 0-20% enzyme activity. Patients with severe MTHFR deficiency may have developmental delay, motor abnormalities, high levels of homocysteine, seizures, and other neurologic impairment. They will also have low levels of methionine in their blood.
The flu can be a real problem for some people so we want to be very aggressive with our therapy in order to minimize the duration & severity of the illness or prevent it altogether.
Take a look at our post on the flu shot to discover why getting your flu shot is a waste of time.
So, if getting the flu shot is a bad idea then what SHOULD we do??
Optimize the immune system
If you read the post ‘What is the flu?’ then you have an understanding of how the influenza virus infects cells. However, your fate is not sealed if you are exposed to the influenza virus. Clearly, not everyone that is exposed to the influenza virus contracts the flu. Well then, who gets the flu? Quite simply, those who’s immune system is weakened for one reason or another. So, the best thing you can do to prevent the flu is to ensure that your immune system is functioning at its highest levels.
Lifestyle Factors
* Avoid sugars, fructose, and grains – Americans consume 75 grams of fructose per day on average. This amount of fructose & sugar can decimate your immune system!
One way that fructose & sugar can have this effect is the impact on gut flora balance. These sugars feed the unhealthy bacteria, and especially Candida, which diverts the attention of the immune function to fight these issues leaving you vulnerable to influenza attack. Our post on gut health talks about this more but 70-80% of the immune function lives in the gut. Any impact on the gut makes gut health absolutely critical for your immune system to function at peak performance! Stick to less than 15 grams of fructose per day.
Also, don’t forget that low blood sugar levels (which often follows high blood sugar & high insulin levels) can be a potent stimulus for cortisol. Elevated cortisol levels depress immune function.
* The 3 R’s – this issue is so important that it is one of the tenants in the ‘Healthy Trinity’. The 3 R’s include Rest (sleep), Recovery from Exercise, and Reducing stress.
There is a lot that goes on behind the scenes when it comes to sleep and what all it does for you. Suffice it to day that lots of sleep can help optimize the physiology and improve hormone (including cortisol) levels which can help improve immune function. Mama was right… rest and chicken soup!
Excess stress can wreak havoc on the body and the immune system. We want to minimize these effects as much as possible. You can read more about these effects on the Adrenal Fatigue post. If you are experiencing mental or emotional stressors then your immune defenses may be a little worn down as well. Dealing with these stressors in an appropriate way can maximize immune function. We have had excellent results with Revolution.calm and several other supplements to help mitigate stress.
* Exercise – Exercise has many benefits for improving your overall health. One of these benefits is that exercise can have a hormetic effect. That means that exercise induces a little stress which stimulates our bodies ability to deal with these stressors. This response persists after stopping exercise which improves our stress adaptability.
Additionally, exercise improves circulation and lymphatic flow. Both of these can be very important for optimal immune function.
* Wash your hands regularly – the influenza virus is susceptible to detergents and frequent handwashing during times of increased exposure can dramatically reduce your exposure to the virus.
Vitamin D
Vitamin D has several effects that help modulate the immune system and reduce the likelihood of contracting respiratory illnesses like the flu. It is very interesting to note that the influenza virus exists year-round but the incidence of illness increases during the winter when our sun exposure is lowest with correspondingly lower levels of Vitamin D. Dr Cannell does an excellent job of laying out the Vitamin D argument in his paper. There are several sources that discuss the evidence linking Vitamin D deficiency and the incidence of flu and colds.
Vit D & URI in Finnish Men – Subjects with serum Vitamin D concentrations < 40 nmol/L had significantly more days of absence from duty due to respiratory infection than did control subjects
Vitamin D and URI – “Serum 25(OH)D levels are inversely associated with recent URTI. This association may be stronger in those with respiratory tract diseases.”
The Vitamin D Connection to Pediatric Infections – “The connection among vitamin D, infections, and immune function in the pediatric population indicates a possible role for vitamin D supplementation in potential interventions and adjuvant therapies.”
Vitamin D Prevents Flu A – “This study suggests that vitamin D3 supplementation during the winter may reduce the incidence of influenza A, especially in specific subgroups of schoolchildren.”
Vitamin D has been shown to be effective in reducing the incidence of influenza in school children. This study also showed a reduction in asthma attacks. These effects were increased if the children hadn’t been taking Vitamin D before and they were starting nursery school after age 3.
Ensuring appropriate Vitamin D levels is probably the most important and cost effective action you can take in order to prevent the flu.
Echinacea
Echinacea has been shown to inactivate the flu virus at recommended dose concentrations. It also has antioxidant and anti-inflammatory effects. A pretty good overview of echinacea is listed here.
Garlic
Garlic is significantly effective in supporting and maintaining healthy immune function. Dr Mercola recommends Garlic for immune support in his post. This post discusses the benefits of garlic pretty well and is well reference.
This article shows benefit for the common cold. A soup made of garlic is suggested to “defeat colds, flu, and even norovirus” in an article in Preventdisease.com. An article on LiveStrong states “Bryan Rade, a naturopathic doctor who practices in Halifax, Nova Scotia, claims that raw garlic is highly effective in warding off the flu.”
We recommend GarlicRevolution due to fact that it is a pharmaceutical grade source of garlic extract. Take 1-2 capsule per day during the flu
EGCg
Epigallocatechin Gallate (EGCg) is a polyphenol in green tea. A study performed in Tokyo showed “that EGCg contained in green tea has potential to inhibit flu infection regardless of its type, and suggested once again that green tea is effective in preventing flu.” Gargling green tea dramatically decreased the incidence of flu (1.3% vs 10%) in nursing home patients in this study. A specific formulation of Camella senensis decreased flu and flu-like illness as well as duration of illness in this study. Or, how about this study on Health Care Workers showing a decreased incidence and duration of clinically defined flu.
Green tea consumption is inversely associated with the incidence of influenza infection among schoolchildren in a tea plantation area of Japan: “Our findings thus suggest that the consumption of 1-5 cups/d of green tea may prevent influenza infection in children.”
Andrographis
Among the many uses of this Ayurvedic and Traditional Chinese Medicine (TCM) bitter herb are that it supports the body’s response to a variety of foreign challenges and helps regulate the body’s temperature during illness. Andrographolides are the major active constituents. Some preliminary research suggests that the herb may stimulate synthesis of antibodies and phagocytosis by macrophages. In addition to the properties above, andrographolides are believed to protect the liver and promote bile secretion. Clinical research has demonstrated an improved sense of wellness in as few as two days after the beginning of supplementation. A three-month study examining andrographis as immune support against foreign microbial challenges demonstrated it was twice as effective as placebo. In clinical trials, 100 mg of a standardized extract of andrographis taken twice daily was sufficient to improve immune response against harmful microbes.
Research indicates that orally administered yeast beta-glucan is processed by macrophages, with subsequent increases in phagocytosis, selective cytokine release, and oxidative degranulation. Macrophages degrade beta-glucan into small fragments that are then bound to neutrophils (granulocytes). This action primes the neutrophils and enhances their ability to eradicate microbial challenges. Prophylactic administration of beta-glucan promotes production of antioxidant enzymes and assists in ameliorating microbial imbalance. Sustained release of beta-glucan fragments into bone marrow may affect white blood cell recovery, a unique mechanism of action exhibited by beta-glucan.
A randomized, double-blind, placebo-controlled trial was conducted during the peak of seasonal immune challenge. Subjects receiving 250 mg of WGP had a significant reduction in the number of days in which signs of immune distress were experienced. A 12-week, randomized, phase II, double-blind, placebo-controlled trial of 1,3/1,6 beta-glucan from S cerevisiae confirmed that long-term use was well tolerated and supported immune system function.
We recommend 250mg of WGP daily during high-risk times of the year for prophylaxis. This is available in Immune Max in our office.
Vitamin C
Vitamin C has long been touted as very good for colds and flu. A Chinese study showed flu virus elimination in vitro (in the lab). Another study showing effectiveness for treatment and prevention. The list of studies showing effect goes on an on. Conversely, Vitamin C has its skeptics as well. The issue is that the only known side effect to oral vitamin C is possible diarrhea but all you have to do is decrease the dose. So there are lots of potential benefits and no real side effects. So, Vitamin C is on my list for colds and flu.
Olive Leaf extract from the traditional medicinal plant Olea europaea, has been shown to possess an array of healthful attributes, including antioxidant properties and effective immune support against opportunistic microbes. Olive leaf’s multifaceted effects on the immune system include the ability to stimulate phagocytosis (an immune response against harmful microbes) and neutralize production of reverse transcriptase and protease enzymes that can adversely alter the ribonucleic acid (RNA) of healthy cells.
Oleuropein, a bitter glycoside that was isolated from olive leaf in the late 19th century, was found to be further hydrolyzed in the body to elenolic acid, which is believed to be its most active component. Research reveals that both olive leaf extract and oleuropein exert positive immune effects, but olive leaf acts in a dose-dependent manner; that is, the greater the dose of olive leaf, the greater the inhibition of microbial replication. Immune Max provides concentrated olive leaf extract that is standardized to 20% oleuropein, while less concentrated formulas are standardized to as little as 6% oleuropein.
What to do if you are required to take the flu shot?
The Following was composed by Dr. Russell Blaylock as a method to reduce autoimmune reactions to the flu vaccines only. Do not use this if you have the flu itself. These are just general observations and not medical advice. You should work with your doctor for a specific program.
Treatment for Toxic Vaccine Exposure
Place a cold compress on the site of the injection immediately after the injection and continue this as often as possible for at least two days. If symptoms of fever, irritability, fatigue or flu-like symptoms reoccur — continue the cold compresses until they abate. A cold shower or bath will also help.
Take krill oil as a source of animal based omega-3 fats.
Curcumin, quercetin, ferulic acid and ellagic acid as a mixture — the first two must be mixed with extravirgin olive in one teaspoon. Take the mix three times a day (500 mg of each)
Vitamin E (natural form) 400 IU a day (high in gamma-E)
Vitamin C 1000 mg four times a day
Astaxanthin 4 mg a day
Zinc 20 mg a day for one week then 5 mg a day
Avoid all immune stimulating supplements (mushroom extracts, whey protein) except beta-glucan — it has been shown to reduce inflammation, microglial activation and has a reduced risk of aggravating autoimmunity, while increasing antiviral cellular immunity.
Take a multivitamin/mineral daily (one without iron — Extend Core)
Magnesium citrate/malate 500 mg of elemental magnesium two capsules three times a day
Vitamin D3:
All Children — 5000 IU a day for two weeks after vaccine then 2000 IU a day thereafter
Adults — 20,000 IU a day after vaccine for two weeks then 10,000 IU a day thereafter
Take 500 mg to 1000 mg of calcium citrate a day for adults and 250 mg a day for children under age 12 years.
We’ll often hear people say they have the flu anytime the get sick with nasal congestion, aches, and a low-grade fever. Sometimes it is hard to differentiate the common cold from the flu. So what is the real deal on the flu?
The flu is an infection caused by the influenza virus. We’ll discuss a little more about what the flu virus is, its characteristics, and the illness it causes in this post. You can read about the flu shot (immunization) here.
The word ‘influenza’ comes from the Italian ‘influentia’ (influence) due to an ancient belief the sudden onset of flu epidemics were due to the the influence of some extraterrestrial force.
When we talk about the ‘flu’ we could be talking about the flu as an illness or the flu as a virus.
The ‘flu’ as an illness
The flu is an illness characterized by these symptoms:
The flu, though it seems bad and is very uncomfortable, is generally a mild & self-limited illness. However, there can be complications from the illness. Complications of influenza virus infection include:
Primary viral pneumonia (influenza)
Secondary viral pneumonia (caused by a different virus such as adenovirus)
Secondary bacterial pneumonia
Myositis and cardiac involvement
Neurological syndromes, e.g. Guillan-Barre Syndrome
Encephalopathy
Encephalitis
Reye’s Syndrome – this is why kids shouldn’t take aspirin for a fever
Allen Smith contracted the Swine Flu and had quite an extreme response. Fortunately, thanks to high-dose vitamin C, he is alive and well today. Here is a video of his story:
How does flu cause the illness?
The influenza virus can establish infection of the upper and lower respiratory tract.
The systemic symptoms noted with the flu are due to the inflammatory response the body mounts due to the infection. Part of this response involves the release of interferon and lymphokine. The interferon and cell-mediated responses (NK and T cells) are very important for both immune resolution of the virus and immunopathogenesis. Some medications (tylenol, anti-inflammatory medications such as ibuprofen) that we take to control symptoms of the flu can inhibit this inflammatory & immune response and can reduce the body’s ability to fight off the virus. This is why I often do not recommend medications to treat fever under most circumstances.
There is a layer of epithelial cells that line the entire respiratory tract from the tip of the nose to the bottom of the lungs. They have specialized functions such as cilia that help move particles out of these areas and mucus secretion. The local symptoms, such as coughing, are due to damage to these specialized epithelial cells. These cells are important for optimal function and protection.
People who have the flu are at higher risk for bacterial superinfection because of the loss of natural barriers and the induction of bacterial adhesion to the epithelial cells due to the damage stated above. Antibody production appears to be important for future protection against infection and is specific for epitopes on HA and NA. We’ll talk more about this stuff below but you can also read more about it in the flu shot post.
How is the flu spread?
The flu is generally spread through the air by aerosolized, infected particles from the coughs or sneezes of infected patients. The airborne aerosols are thought to be the most common mode of transmission but we don’t know for sure. Influenza can be spread directly by contact with nasal secretions or bird droppings. The infected material can be deposited on surfaces such as door knobs.
The influenza virus is inactivated by sunlight (UV light), disinfectants, and detergents. Since detergents (soap) are effective against the influenza virus frequent handwashing may help reduce the risk of infection.
Infected persons begin shedding new virus particles the day before symptoms develop and shed new viruses for 5-7 days. Thus, they are contagious BEFORE they have symptoms.
How do we diagnose the flu?
First, not everyone needs to be tested. One of the primary reasons to test is that some physicians may prescribe anti-flu medications if you have had symptoms for less than 48 hours.
Rapid Influenza Diagnostic Tests (RIDTs)
These tests can help diagnose flu in patients who have signs and symptoms consistent with the flu. They can also help determine if outbreaks of respiratory illness are due to influenza (i.e., nursing homes). In general, rapid diagnostic testing for influenza should be done when the results will affect clinical decision making.
These tests can detect Influenza A & Influenza B. They take less than 30 minutes to perform and are accomplished by obtaining a nasal swab, wash, or aspirate. They may or may not differentiate the type of flu present but they don’t give detail about the strain (H1N1, H3N5, etc).
The false negative rate (when the test is negative but you really do have it) is relatively high but false positives can also occur.
These tests are immunoassays in order to detect the flu virus.
Virus Isolation
We can isolate influenza flu virus particles from respiratory secretions. We obtain a direct aspirate, gargles, or nasal washings. These samples are then examined by immunofluorescence of the exfoliated cells. They can also be inoculated in cell cultures or embryonated eggs.
Serum antibodies can be assessed by hemagglutination inhibition.
Diagnostic Methods
Cell culture in primary monkey kidney cells for the presence of virus
Hemadsorption to infected cells for the presence of hemadsorbing virus
Antibody inhibition of hemadsorption for the presence of influenza, type, and strain
Immunofluorescence, ELISA – Influenza virus antigens in respiratory secretions or cell culture
Hemagglutination – presence of virus in secretions
Hemagglutination inhibition (HI) – type and strain of influenza virus
Serology: this form of testing is not recommended
Epidemiology
Influenza A is essentially an avian virus that has “recently’ crossed into mammals. Birds have the greatest number and range of influenza strains. Avian hemagglutinins sometimes appear in pig, human, and horse influenza strains.
About every 10-15 years a major new pandemic strains appears in humans, with a totally new HA and sometimes NA as well (antigenic shift). The new variant causes a major epidemic around the world (pandemic).
This strain undergoes minor changes (antigenic drift) every 2 years. This is probably driven by selective antibody pressure in the populations of infected humans.
Influenza A Evolution
1874 – H3N2
1890 H2N2 Pandemic
1902 – H3N2
1918 – H1N1 Pandemic
1933 – H1N1 First strain isolated
1947 – H1N1 Variation detected (antigenic shift)
1957 – H2N2 “Asian” flu pandemic
1968 – H3N2 “Hong Kong” flu pandemic
1977 – H1N1 “Swine” flu, Fort Dix, non-epidemic
1978 – H1N1 “Russian” flu epidemic
1983 – H3N2 “Philippines” flu pandemic
2000 – H3N2 “Sidney” flu epidemic & H1N1
Influenza B epidemics occurs in Influenza A ‘off’ years. Influenza B often co-circulates with Influenza A.
This constant antigenic change down the years means that previous flu vaccines are not effective against new strains. Thus, new flu shots are formulated on a regular basis. New influenza strains spread rapidly in daycare centers and schools and in places where people crowd together. Influenza epidemics may cause significant economic losses due to high morbidity and mortality rates.
Because another devastating pandemic strain (1918 pandemic killed 20-40 million people worldwide) may appear any time, the World Health Organization (WHO) maintains worldwide surveillance of influenza strains and makes predictions of suitable strains for vaccine production.
Small clusters of human infections with avian influenza type A (H5N1) and (H9N2) occurred in Hong in 1997-98 from contact with infected fowl. So far, none of these strains have become established in humans. However, the incidence caused worldwide concern about the possible emergence of new “killer” influenza virus strains and intensified influenza research and vigilance programs.
The flu as a virus:
Viruses are bits of RNA or DNA that are able to incorporate into cells and cause damage or alter the function of those cells. They are not technically living and are unable to replicate or reproduce on their own.
Virus structure:
Influenza is a spherical shaped, enveloped virus. The virion is the complete form of the virus outside of the host cell and consists of the RNA, protein coat, and lipid envelope. The nucleocapsid is the RNA plus the protein coat. It is what remains once the lipid envelope is removed.
Influenza is a negative ss-RNA genome of 8 separate segments, nucleoprotein (NP) and 3 polymerases. The ‘negative’ ss-RNA means that the virus genome is RNA in a single-strand form (ss) which encodes for mRNA.
The nucleocapsid is enclosed within an outer lipoprotein envelope which carries 2 protruding spikes. One spike is a box-shaped protein called the neuraminidase (NA) which has properties of an enzyme (as the -ase at the end of the name suggests). The function of the neuraminidase (NA) assists with movement of the influenza virus particles through the respiratory tract mucus and the release of the virus particles from the infected cells. There are 9 major antigenic types of NA (1-9).
The other envelope spike is a trimeric protein called the hemagglutinin (HA). There are 13 major antigenic types of HA. The hemagglutinin functions during the attachment of the virus particle to the cell membrane. It combines with sialic acid receptors on a variety of cells including red blood cells and epithelial cells.
Thus, H1N1 virus has HA type 1 and NA type 1.
Inside the virus envelope is an ill-defined antigenic protein called the Matrix Protein (MP). The lipoprotein envelope of the influenza virus makes the virion susceptible to heat, drying, detergents, and solvents.
Classification: Orthomyxoviridae
The classification of influenza is done on the basis of antigenicity of NP and HA into 3 main groups:
Influenza A: HA & NA undergo minor and occasionally major changes. It can be the cause of epidemics and pandemics
Influenza B: Relatively slow changes in time. Influenza B is only seen in humans. It can be the cause of epidemics.
Influenza C: Uncommon, filamentous strain that is only seen in humans. Typically there are only sporadic cases of Influenza C.
Influenza is named by this nomenclature: A/Singapore/6/86/H1N1
This means: Influenza A / Town where it was first isolated / Number of isolates / Year it was isolated / Major type of HA & NA
How does the virus replicate?
Influenza is a receptor-bound virus and is taken into the cell by endocytosis. This is a process by which the cell ‘swallows’ or engulfs the virus. Once inside the cell, the envelope of the virus fuses with the lipid bilayer of a vesicle and releases the viral RNA. Thus, the virus is unwrapped and this process is called uncoating.
When the virus is making new viral proteins they are translated from transcribed mRNA. New viral RNA is encased in the capsid protein which is then transported to cell membrane batches which have been modified by viral Matrix Protein (MP) and the HA and NA spikes membrane proteins. The underlying MP acts as a homing device, so to speak, for the nucleocapsids.
The new virus particles are formed inside the cell and are released from the cell by a process called budding. The cell does not die in this process. At least not initially.
The influenza virus has a segmented genome structure. This means that there are ‘chunks’ of RNA that can act, or be acted upon, separately and can reorganize their structure when a cell is infected with 2 different viral strains. This structure greatly increases the recombination potential and contributes to the rapid development of new virus strains in nature. The reassortment process is duplicated in the lab for making flu immunization strains.
Avian and human strains combining in pigs in the Far East are the main source of new virulent human strains. This is why we (Americans) go to Asia when we are looking for which influenza strains may be spreading to the US for selection in the flu shot.
Emergence of new influenza virus strains
New influenza virus type A strains arise by recombination between human and animal strains as stated above. This is called ‘antigenic shift‘. In contrast, type B influenza virus strains arise by point mutation which is called ‘antigenic drift‘.



 There is a lot of attention on testosterone these days. There are lots of Low T clinics popping up all over the place.
There is a lot of attention on testosterone these days. There are lots of Low T clinics popping up all over the place.
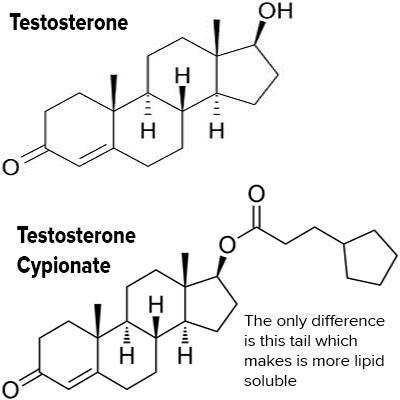
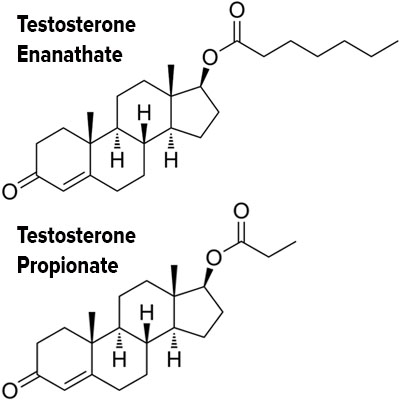
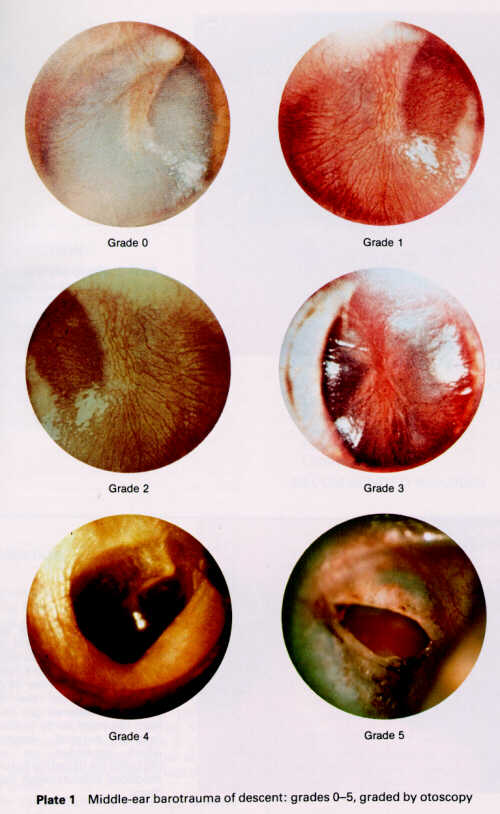
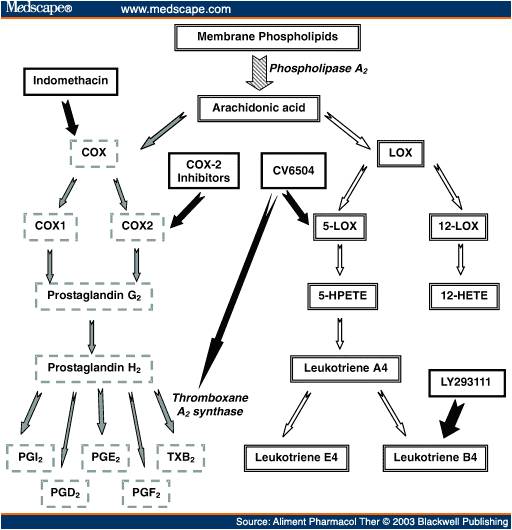





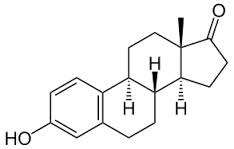
 This post will be an introduction to iodine and we’ll follow with information about how iodine specifically affects things like breast & prostate cancer and thyroid disease in additional posts.
This post will be an introduction to iodine and we’ll follow with information about how iodine specifically affects things like breast & prostate cancer and thyroid disease in additional posts.