How do you get Coronavirus Treatment in Tulsa, Oklahoma?
I’ve been reading all of the ‘hype’ about this virus and I decided that I had to say something about it. I’m blown away at how ridiculous this whole thing has become. You may or may not know that, in addition to seeing patients at Revolution Health (our Tulsa, Oklahoma Functional Medicine Clinic), I also work in the Emergency Room. In fact, I’ve worked in over 10 different Emergency Rooms over the last 13 years and I’ve seen a lot of stuff.
One of the more common issues I’ve seen in virtually every Emergency Department is related to flu like illness or the common cold. The vast majority of these patients do not need an Emergency Department evaluation and nothing is done for them except tylenol or ibuprofen for symptom management. Keep in mind that these patients almost never have breathing difficulty, hypoxia (low oxygen levels), or any other signs of a severe illness. They simply feel bad and they have a fever, cough, runny nose, body aches, etc.
In the absence of severe illness, these patients DO NOT need to be seen. Some may want the medication for influenza, Tamiflu. Check out my podcast about Tamiflu if you want more information about that. Some hospitals have a respiratory panel available. This is typically a PCR test which is able to detect and identify a handful of viruses (rhinovirus, influenza, RSV, adenovirus, etc) which could explain symptoms. However, the results rarely change our management other than providing information on how patients may limit exposure to others.
I’ve seen a number of different virus “scares” over the years. You may recall Swine Flu in 2008-2009. SARS (Severe Acute Respiratory Syndrome) was a big concern in 2003. Interestingly, SARS was due to a novel Coronavirus though not the same as SARS-CoV-2 currently in the spotlight for causing COVID-19.
Coronaviruses have been around for a long time and are responsible for up to 1/3 of all upper respiratory tract infections (common cold type illnesses).1-3 However, COVID-19 seems to affect more people, be more transmissible, and have more potential for severe illness than the common cold.
How is the Coronavirus (COVID-19) transmitted?
The primary method of transmission is person to person though respiratory droplets. That means that an infected person coughs, sneezes, or breathes droplets of respiratory secretions which contain the virus and distributes them into the air. These airborne droplets then come in contact with another person who could contract the virus.
While it is believed that the virus can be transmitted by touching a surface that has the virus on it and then touching your face (mouth, nose, eyes, etc), it is NOT thought to be a primary means of transmission.
The virus is likely most transmissible when a person is at the height of their illness. However, they MAY be able to transmit the virus before they know they may have it.
The incubation period for COVID-19 appears to be less than 14 days with most cases exhibiting symptoms around 5 days after exposure.5,6
What happens if I get the Coronavirus (COVID-19)?
In many cases, it is the same as the common cold. That is one reason that I believe the hype around all of this Coronavirus hysteria is a bunch of hogwash!
Initial reports from China demonstrated that 6.1% of patients having COVID-19 were admitted to the ICU (5%), put on a ventilator (2.3%), or died (1.4%). Fever was the most common symptom – 43.8% of patients who were admitted but the number increased to 88.7% during their hospitalization. 67.8% of patients had a cough.5 It is important to keep in mind that most of the sicker patients were elderly or immuno-compromised.
Let me be very clear here, only 2.3% of patients required a ventilator. Only 1.4% died. Death to any patient is a bad thing but the fear mongering about this virus has gotten totally out of control! For example, an article published in The Atlantic painted the picture that the disease is so severe in Italy that hospitals and physicians are being completely overwhelmed.7 At the time of this writing (the same day of the Atlantic article by the way), there are over 10,000 cases of COVDI19 in Italy with 631 deaths. While this death rate is 3 times higher than that in China, it is still only 6.3%.
If the Wuhan data is also true for Italy then there are only 230 patients on a ventilator due to COVID19 in Italy. Even if it is 3 times higher, as is the mortality rate, it is 690 patients. This is much lower than Mr Mounk would lead you to believe in his Atlantic article. While 690 patients on a ventilator is too high, it is just not the medically overwhelming numbers stated. This is just another example of the hyper-inflated, biased approach with which the media is delivering information and it isn’t doing any of us any favors!
A word of advice: if you have any of the symptoms but have no evidence of severe disease then stay home! It may be helpful for epidemiologic purposes to have a diagnosis but it won’t make any difference (in most cases) to know you have it.
There is a complete lack of education on how to handle acute viral illness such as flu, common cold, COVID-19, or any other acute upper respiratory infection. There are no specific treatments for these infections so there is little need to go to the doctor just to get a diagnosis unless you have a severe disease requiring hospitalization. Just because you (or your child) have a fever does NOT mean that you need to go to the ER!
What can I do if I am exposed or actually have Coronavirus?
As stated previously, there are no specific treatments or cures for SARS-CoV-2. Treatment is symptomatic. That simply means that you treat the symptoms. There simply isn’t much that we (doctors) do for many of the symptoms until you are severely ill.
For Severe Illness:
What is severe illness? The full definition is beyond the scope of this article but suffice it to say that you can’t breathe, your oxygen levels are declining, your level of consciousness is declining, and so on. These are the kind of symptoms that would get you admitted to the hospital, placed in the ICU, or put on a ventilator.
For Non-Severe Illness:
What is non-severe illness? Basically, it is everything else. Fever, cough, runny-nose, fatigue, body aches, etc. If these symptoms remind you of the flu then you are right. The reason is that these symptoms are the body’s immune response kicking in to a viral infection. That is why it is so hard to tell between the flu and the common cold. The body responds to many of these viruses in the same way.
There are no specific treatments or cures for the Coronavirus or COVID19. However, there ARE things that you can do that may help your immune system better fight the virus. The better your immune system works the better it an fight the virus. Therefore, our recommendations are based around optimizing your immune system as well as your overall health.
Recommendation #1: lower stress, get plenty of sleep, and get moving (exercise).
Recommendation #2: Garbage in, garbage out. Get rid of the garbage! Eat good, high-quality foods. Be sure to get plenty of fruits and vegetables. Follow the Revolution Nutrition plan.
Recommendation #3: Zinc Glyinate 20mg daily. Zinc plays a critical role in multiple biological processes. It has critical roles in the immune process as well. In fact “Recent studies have demonstrated that zinc supplementation can significantly reduce the morbidity and mortality of apparently well-nourished children and shorten the time to recovery from acute infectious diseases.8” Now here is a VERY interesting piece of information. Zinc blocks the replication of Coronavirus in vitro9 (in a petrie dish).
Recommendation #4: NAC 600mg twice daily. N-Acetyl Cysteine is an antioxidant and at least one study shows that it can decrease the inflammatory response to community acquired pneumonia. This particular study described the oxidative damage that occurs with viral pneumonia and how the antioxidant systems are quickly overwhelmed.10 NAC appears to blunt this affect. NAC is also a mucolytic meaning that it helps break up secretions.
Recommendation #5: Vitamin C 2 grams daily. That is, of course, if you are taking it orally. Unfortunately, there is a limit to our gastrointestinal absorption so if you take more than you can absorb then it just passes through (with some uncomfortable bowel side effects.
The real benefit is with IV Vitamin C. The serum levels are orders of magnitude higher than oral. We’ve been using IV Vitamin C for years at Revolution and our patients love it. I’ve noticed tremendous benefit myself with acute illness such as the common cold or flu-like illness.
While there are no studies showing benefit with coronavirus we do know that Vitamin C has had significant benefit on viral and bacterial infections. There is a lot of information about Vitamin C in this paper: Vit C – 42 year stonewall.
Recommendation #6: Immunotix 500 1 capsule daily. Immunotix is made with whole glucan particle which has been shown to have positive immune supporting effects. Research has shown that these glucan particles “prime” neutrophils and make them better able to provide support against microbial challenges.11
Recommendation #7: Viragraphis 1 capsule twice daily. Viragraphis is a supplement containing 3 separate herbs which may support immune response, maintains healthy lung tissue, and supports a healthy response to inflammation. Andrographis, one of the herbs in Viragraphis, was shown to be “effective in reducing symptoms of upper respiratory tract infection” in one study.12 The other 2 herbs, Licorice Root Extract and Isatis indigotica, also provide immune support and upper respiratory tract health.
Recommendation #8: Xcellent A 7500. “Vitamin A deficiency results in multiple derangements that impair the response to infection.”13 While this study didn’t prove that Vitamin A supplementation treats viral illness, it is clear that vitamin A deficiency contributes.
Recommendation #9: Consider other interventions such as Vitamin D, Argentyn 23, Olive Defense, Elderberry, and many other possibilities. They are worth a shot.
Finally, there is an experimental drug, DRACO, which “could cure nearly any viral infection” according to MIT News. Unfortunately, continued research was halted due to a lack of funding. That just sounds ludicrous as it may be just what the doctor ordered.
Summary
In summary, the hype around this virus is ridiculous. Certainly, we should take REASONABLE precautions and protect those at risk. However, shutting down entire countries, cancelling all of these events and gatherings, and countless other knee-jerk reactions just seems asinine.
We should do everything we can to be as healthy as possible and we need to be comprehensive in our approach.
If you have nasal congestion, seasonal allergies, cough, sore throat, ear congestion & pain then this is the plan for you. I’ve seen excellent results with this plan.
General Instructions: These medications are topical medications and exert little to no systemic effects.
Because of the anatomy of the nose, you want to get the medication to the lateral (outside) wall of your nose. The best way to do this is to ensure that you spray the medication at a 45o angle up and 45o angle out – you don’t want to spray the medicine toward the middle of your nose. I generally recommend using your right hand to spray the left nostril and vice versa – this helps to achieve the proper angle.
Lean slightly forward and take a very small sniff as you spray the medicine. If you can taste the medicine, you sniffed too hard or sprayed too flat.
Afrin: This is a topical decongestant that you can purchase over-the-counter (OTC) or may have been prescribed and available at the pharmacy. The generic is as effective as the brand name. In my experience, Neo-Synephrine, Afrin, and Oxymetazoline are all equally effective though you may find one that you prefer.
Follow the “General Instructions” above for the proper procedure
Use one spray in each nostril, wait about 5 minutes and then repeat. The purpose is that the nasal respiratory tissue is congested and the medication can’t get to all of the surfaces. Using 1 spray starts the decongestion so that when you spray the 2nd, after several minutes, the tissues have started to open up and the medication can then get to more of the tissues and you have a better effect.
This medicine is extremely effective and starts to work immediately. You may use it up to twice daily for a maximum of 3 days!! It may not last a full twelve hours but don’t use it more than twice daily. You don’t have to follow a strict 12 hour schedule and you can use it at the times when you’ll benefit from the decongestion the most, such as just before going to bed.
Take at least 3 days off before you start to use it again if needed.
Use of this medication for more than 3 days can lead to worsening congestion that requires more and more decongestants – a condition called Rhinitis Medicamentosa. This is a difficult condition to treat.
You may take oral decongestants in addition to this medication without interactions.
Neilmed Sinus Rinse: One of my favorites. It is available OTC at pharmacies but may also have been prescribed. It is merely a saline solution and is a “bath for your nose.” It has some good research that backs up its effectiveness and I have never had a patient tell me that they didn’t benefit from it. It may feel a little weird but is not painful. I generally recommend using the Afrin and then waiting for about 30 minutes if you are congested to help open things up before rinsing. I recommend 2-3 times per day but may be used as often as you wish.
Flonase: or other inhaled topical steroid. Most of these are now available over-the-counter. There are others on the market but this one is the most potent steroid – personal preference may dictate a different steroid. The instructions below apply to all of them.
Follow “General Instructions” above – this should prevent one of the adverse effects of chronic use, nasal septal perforation.
This medication is for chronic use and should not be used on an “as needed” basis because it takes 4-6 weeks to get full effect from it
You should either wait about 30 minutes after using this to rinse your nose with the Sinus Rinse or use this after rinsing your nose.
You may start with 2 sprays per nostril but you can probably cut down to one spray per nostril per day after a couple/few weeks.
The healthiest people I know all exercise regularly. And most of them exercise with a lot of intensity. The most unhealthy people I know don’t move much at all much less exercise. If you want revolutionary health then you absolutely must exercise.
Many patients at our Tulsa Functional Medicine clinic are interested in exercise but they don’t know exactly what to do. There are lots of exercise programs – P90X, Insanity, traditional weight lifting, aerobics (running, bicycle, elliptical, etc). What should you do?
Exercise is vital for overall health and it has very little to do with burning calories. However, the KIND of exercise can make all the difference in the world!
I’m sure you’ve seen someone who ran 20 miles a week and still didn’t lose weight, it might even have been you. Burning calories is not what causes weight loss. Ironically, it also doesn’t have as much to do with how much you eat either but that is another topic.
If it isn’t how many calories you eat and how many calories you burn through exercise then what is it?
First, the DNA…
Within the nucleus of every cell in your body (except red blood cells) lies the master control center: DNA
Your DNA controls cellular function. It encodes for the proteins and functions needed for the cell to do what the cell is supposed to do. You can think of your DNA as a reference or “how-to” manual for the cell. The problem is that your cells do not live in isolation. They live within a changing, and often, toxic environment. They are constantly under attack by bacteria, viruses, oxidative stress, toxins, and numerous other factors that can harm or even kill them.
Cells get damaged. Frequently. And when they do they need to fix themselves. DNA is not only the “how-to” manual for the cell but it is also the “repair manual.”
Our bodies, our cells, are under constant attack. We live in a toxic environment. We eat crappy foods. We are overly stressed. We are frequently exposed to numerous toxins such as heavy metals, environmental pollutants, pesticides, and countless chemicals. The more toxic our exposures the more damage we incur. We need mechanisms to repair our cells.
The human body contains 20,000-25,000 genes.1 Genes encode for proteins which control cell function and repair. However, most of your DNA does not encode for proteins. Instead, these regions regulate gene expression – when genes are turned on or turned off.
You have all of these genes but most of them are dormant at any given time. Genes are only accessed when needed by the cell. You may have a repair manual for your car but you may not ever need the page (instructions) for ‘how to change a lightbulb.’ You have to have a need for that page, open the book, and follow the instructions. Cellular damage of different types stimulates certain genes to facilitate their repair.
This is how DNA works. When the conditions are right the cell turns to the specific gene for the instructions for that need. Turning on some genes is a bad thing. For example, if you have the genetic SNP for 9p21 and those genes are turned on, then you have a 100% increased risk of cardiovascular disease. The cool thing is that you can change cellular conditions and make it where that gene isn’t ever turned on.
Many influences turn genes off and on
These genes are not turned on and off randomly. They are turned on and off when certain conditions are met. Hormones and other cell messengers are the signals that turn these genes on and off. There are many of these cell messengers and there are many reasons they will trigger the response.
Some of these signals come from within the cell but others come from elsewhere. Cell signals, via hormones, are created in other parts of the body and bind to receptors on the surface of cells. Once they bind, they cause a change within the cell.
Hormones and other signals are generated based on the internal and external environment of the body. This means that your nutrition, stress levels, sleep, light and sun exposure, noise, temperature, and even your movement all influence the release of hormones and, ultimately, cellular function. All of this will influence whether certain genes are turned on or will remain silent.
Exercise changes the cellular conditions altering gene expression and changes cell function.
Bioidentical hormone replacement therapy (BHRT) has absolutely revolutionized the health of many of my patients at Revolution Health in Tulsa. I see the benefits on a daily basis. Some patients come back (for follow up) in tears and can’t believe they feel so good after feeling so bad. They often tell me they feel as though they’ve gotten a second chance at life or that they have their life back.
Second only to Prolotherapy, which is probably the single most effective thing I do in my clinic, bioidentical hormone replacement therapy is one of the most effective interventions we offer.
I recall a former nurse of mine who went to see her OB/GYN. She saw a prescription to a local compounding pharmacy and asked the medical assistant what the doctor thought about bioidentical hormone replacement (BHRT). The assistant stated “she thinks its a scam but the patient wanted it.”
A scam.
This concept is simply beyond me. Why on earth would she think it is a scam?!?
I supposed it is because some major medical societies are opposed to bioidentical hormone replacement therapy (BHRT). At first pass this doesn’t make much sense either until you understand what bioidentical hormone replacement therapy (BHRT) is, how it is done, and why they are opposed to it.
What is Bioidentical Hormone Replacement Therapy (BHRT)?
Simply, it is the use of hormones which are bioidentical to human hormones and at doses which are generally customized to each individual patient.
Bioidentical hormones can be fashioned for oral (pills, troches, liquid), transdermal (creams, gels), injectable, and percutaneous (pellet) use. Doses can be individualized for a custom approach for each patient.
The only way to get this level of customizability is to compound these medications at a compounding pharmacy.
By the way, compounded medications are not FDA approved and that is one of the major hang ups these medical societies (ACOG, Endocrine Society, etc) have with bioidentical hormone replacement therapy (BHRT).
Some bioidentical hormone replacement therapy (BHRT) prescribers use a customized approach based on patient symptoms. Some use blood testing. Others use saliva testing or urine testing to tailor the dose to the specific patient.
What exactly does FDA approval mean?
The FDA approves certain medications. Basically, the drug manufacturer performs studies on safety and effectiveness and presents the data to the FDA. The FDA will review the data and either approve or reject it.
It is important to understand that FDA approval means that the company presented data on a specific drug and a specific dose or doses. For example, Testopel (testosterone pellets) are FDA approved in doses ranging from 150-450mg. [1] That is 2-6 pellets. So, technically speaking, 1 single pellet (75mg) is not FDA approved. Additionally, 525mg (7 pellets) is not FDA approved either. Neither of these doses appear to have been studied by the manufacturer so there was no data submitted to the FDA for approval so the FDA obviously couldn’t approve it.
Clearly a 75mg dose wouldn’t be harmful but it may be insufficient to achieve desired results. But, again, it virtually couldn’t be harmful or detrimental. It is also unlikely that the 7th pellet is harmful though I guess it is possible. In any case, use of Testopel at any dose other than 150-450mg is not FDA approved and considered “off label” use.
Physicians do have the authority to use medications “off label” and have done so for years. There are a number of medications that are being used off label.
Clonidine – a blood pressure medication used for ADHD
Namenda – approved for Alzheimer’s disease but used for Obsessive-Compulsive Disorder (OCD)
Propranolol – approved for hypertension but used for performance anxiety
Viagra – approved for male erectile dysfunction being used for female sexual dysfunction
I make no argument against these medications being used off label. In fact, they may be very beneficial in some cases. These are common uses which are generally accepted in the medical community. Additionally, the FDA merely governs drug approval not drug prescribing and physicians are free to prescribe a drug for any reason they believe is medically appropriate.
Non-bioidentical Hormones
Now that we understand a little about how medications are FDA approved we can dig a little deeper into the typical prescribing of hormones. There are FDA approved bioidentical hormones for estrogen, progesterone, and testosterone. However, many hormone prescriptions are for non-bioidentical hormones such as Premarin.
Most traditional physicians prescribing hormones are not customizing the dose to the individual patient. That is another component setting bioidentical hormone replacement (BHRT) apart from non-bioidentical hormone replacement.
Premarin is a great example of a non-bioidentical hormone replacement therapy option. Premarin is available as an oral tablet in 5 doses (0.3, 0.45, 0.625, 0.9, and 1.25 mg). Obviously there is a level of customization available but only in those options. In practice, it has been my experience that many doctors will simply prescribe one dose for most patients. Kind of a “one size fits all” approach. I think it is because they don’t understand how to properly manage the dose and tailor it for the patient.
The Women’s Health Initiative (WHI) study details some of the risks and benefits of using some of the non-bioidentical hormones for post-menopausal women.
The argument against bioidentical hormone replacement therapy
As stated earlier, many doctors and many medical societies are opposed to bioidentical hormone replacement therapy (BHRT).
The American College of Obstetricians and Gynocologists (ACOG) Position Statement on bioidentical hormone replacement states “Evidence is lacking to support superiority claims of compounded bioidentical hormones over conventional menopausal hormone therapy.” [2]
The Endocrine Society stated “‘Bioidentical hormones,’particularly estrogen and progesterone, have been promoted as safer and more effective alternatives to more traditional hormone therapies, often by people outside of the medical community. In fact, little or no scientific and medical evidence exists to support such claims about ‘bioidentical hormones.’ Additionally, many ‘bioidentical hormone’ formulations are not subject to FDA oversight and can be inconsistent in dose and purity.” [3]
I understand that there is not good ‘evidence’ to support a customize approach to hormone therapy but I believe it is very important to ask WHY there isn’t good evidence. What is the typical source of this evidence? The bottom line is that the source is research studies and if you can get randomized, placebo-controlled, double-blinded studies then you have the cream of the crop.
But these studies are very expensive and someone has to pay for them. The only ones, typically, willing to spend the money are those with something to gain. And it needs to be a LOT to gain! Estimated costs to get a prescription drug FDA approval range from $161 million to $1.8 billion dollars. That is a staggering amount of money! Additionally, the data submitted to the FDA have to cover the range and combination of medications seeking approval. Costs will go up exponentially.
Basically, you just have to follow the money to understand how these medications get support.
But let’s talk about compounding for just a minute.
Compounding medications
It is frustrating that the Endocrine Society said that these formulations “are not subject to FDA oversight…” [3] That is simply NOT the case!
The FDA absolutely has oversight over these medications. FDA Regulations 503a & 503b govern compounding pharmacies. Additionally, the state board of pharmacy also behaves as an agent of the FDA, DEA, and the State Board of Pharmacy. In fact, the FDA can walk into any compounding pharmacy at any time and ask to inspect the facility.
With that being said, there is a huge potential for quality concerns with compounding pharmacies. A great example of a poor compounding pharmacy was the New England Compounding Center (NECC). You may recall that several people died several years ago due to infections caused by medications from this pharmacy. I have had experiences with more than one compounding pharmacy illustrating these quality concerns.
One of my staff members was on progesterone when the compounding pharmacy we typically used was bought by another pharmacy. Her next refill after the transfer of ownership didn’t go well. She told me that she felt as though she wasn’t even taking progesterone anymore. Her night sweats returned as well as her other symptoms. She was very frustrated.
We called the pharmacy and they told us they had made some changes and would send another prescription which seemed to fix the problem. However, she got another prescription at a later date and had the same problem. It seemed that every time she got her medication filled at that compounding pharmacy there was a problem but when she got it somewhere else it was fine. That is obviously concerning.
On the other hand, I have used another compounding pharmacy for several years and never had a single problem. I have toured their facility and I know their quality control measures. I know how they seek the highest level of quality and what steps they take to ensure it. There are many pharmacies with the same level of quality and we have had good success with those as well.
If you are wanting compounded medications it is essential that you have a relationship with the pharmacy and know their history OR you know a reputable doctor who knows which pharmacy to use. I have talked with several compounding pharmacists asking them how the average patient knows which pharmacies are good and the bottom line is that you can’t. It is all about the relationship based on history.
The argument about quality variance is the cornerstone to the ACOG’s and Endocrine Society’s statements. Dr Santoro added “The biggest issue is the lack of evidence for safety or efficacy. The available evidence suggests that overdosage and underdosage can be common because of lack of standards in the bioidentical industry.” [4]
Their argument is valid. However, the risks can be easily circumvented when you find a good compounding pharmacy and there is tremendous value added. Unfortunately, these societies are throwing the baby out with the bathwater and ignoring a tremendous benefit. It is a true shame. The FDA has stated that “…compounded drugs can serve an important medical need for some patients…” [6] I believe that this is definitely one of the times when compounded drugs can make a big difference.
Customized Approach
The other reason ACOG and the Endocrine Society are opposed to bioidentical hormone replacement therapy is that they feel there is no evidence to support a customized approach for each individual patient. I can tell you they are wrong.
Their position is that there are no STUDIES proving that a customized approach is more beneficial. However, you will likely never see any studies proving this information. Why?
First, reference my discussion above about following the money trail. These studies are launched by people who have something to gain by funding a study. No money, no study.
The second reason you won’t see studies validating a customized approach is that you can’t standardize the approach. It is very difficult to ensure that all patients get the same level of therapy but still have a standardized approach. One way to do this would be to treat to a certain ‘level.’ Yet there is no consensus regarding treatment levels making this a very difficult concept to achieve.
Also, many of my patients had been on hormone replacement when they came to me. Countless women had been on different forms or doses of estrogens, progesterone (or progestins), and/or testosterone. Yet many of these patients were still having symptoms and didn’t feel well. Once we switched them over to bioidentical hormone replacement therapy (BHRT) they nearly instantly felt better.
How can we, in good conscience, tell patients that, despite the fact that they feel better, there is no evidence to support continuing their therapy? It just doesn’t make sense to me. Additionally, there is absolutely no evidence of harm. No study shows harm with the use of bioidentical hormone replacement therapy (BHRT).
No evidence of harm. Evidence showing benefit.
Bioidentical Hormone Replacement Therapy (BHRT) is Beneficial!
Bioidentical hormone replacement therapy (BHRT) is a valid, safe, and effective therapy that can help a lot of people!
As stated previously, the ACOG and Endocrine Society (among others) state that there is no evidence of benefit. Stated again, the Endocrine Society said that bioidentical hormones “have been promoted as safer and more effective alternatives to more traditional hormone therapies, often by people outside of the medical community. In fact, little or no scientific and medical evidence exists to support such claims about ‘bioidentical hormones.’ [3]
However, there IS evidence showing superiority and safety!
Risks associated with estrogen (Premarin) alone include stroke and blood clots. The combination hormone therapy (PremPro) risks include cardiovascular disease, stroke, breast cancer, and pulmonary embolism.
Another study showed a negligible risk of blood clots when non-oral estrogens are compared to oral estrogens. Non-oral estrogens also appear to be beneficial for blood pressure. [7]
They went on to say that “growing literature suggests that the progestins used in association with estrogens may not be equivalent.” [7] “Compelling indications also exist that differences might also be present for the risk of developing breast cancer, with recent trials indicating that the association of natural progesterone with estrogens confers less or even no risk of breast cancer as opposed to the use of other synthetic progestins.” [7]
A study by Simon showed no increased risk of VTE or stroke. He demonstrated that progesterone has no increased risk of VTE or breast cancer. He went on to say “the use of transdermal estradiol and micronized progesterone could reduce or possibly even negate the excess risk of VTE, stroke, cholecystitis, and possibly even breast cancer associated with oral HRT use.” [8]
A study performed in France, called the ESTHER trial, showed that “oral but not transdermal estrogen is associated with an increased VTE risk.” [9] They also noted that synthetic progestins (norpregnane derivatives) may increase blood clots but this risk was not noted with micronized progesterone and pregnane derivatives. [9]
Multiple studies demonstrate superior safety with bioidentical hormone replacement therapy (BHRT) compared to traditional hormone replacement. BHRT is an invaluable tool and it can be life changing for many women.
L’hermite M, Simoncini T, Fuller S, Genazzani AR. Could transdermal estradiol + progesterone be a safter postmenopausal HRT? A review. Maturitas. 2008 Jul-Aug;60(3-4):185-201. doi:10.1016/j.maturitas.2008.07.007. Epub 2008 Sep 5.
Simon JA. What’s new in hormone replacement therapy: focus on transdermal estradiol and micronized progesterone. Climacteric. 2012. Apr,15 Suppl 1:3-10. Doi: 10.3109/13697137.2012.66932.
Canonico M, et al. Hormone therapy and venous thromboembolism among postmenopausal women. Impact of the rout of estrogen administration and progestogens: the ESTHER study. Circulation. 2007;115;840-845.
Bioidentical Hormone Replacement Therapy (BHRT) Pellets are a great option for many of our Tulsa clinic patients. We were very reluctant to offer this procedure for a long time. However, after reviewing all of the data available how Pellets are inserted & managed as well as the quality of pellets it became clear that we simply had to offer this procedure.
Pellet insertion is safe, easy to do, very effective, bio-identical hormone replacement therapy.
Here are some questions to consider:
How often will I need pellets?
For women: usually every 3-4 months.
For men: usually every 4-5 months.
Why are pellets better than creams, patches, shots, or pills? The pellets are pure hormones that are not metabolized into byproducts by going through the liver, stomach or skin. This delivery system allows your body to use the right amount of hormone from the pellet as the blood flow surrounding the pellets picks up what is needed. In a word, it is the most natural and physiologic way to replace hormones.
Where do the pellets go? Because they are pure hormone without fillers or synthetic ingredients, they completely dissolve.
I want to loose weight…How long will it take for my body to get back to lean normal? That depends on how much you exercise and work out with weights, as well as your age. Testosterone decreases fat and increases muscle and lean body mass. Testosterone also increases your natural growth hormone and therefore will improve your stamina to work out and increase muscle mass. Testosterone is optimized with pellet therapy more than any other treatment including creams and injections.
I have no libido. What will Pellets do for that? Optimal bio-identical hormone balance will greatly improve your libido. The addition of testosterone in pellet form will change everything for the better!
I get horrible headaches. Will Pellets help with that? Yes! We have had great success, especially with women who have menstrual migraines, and new migraines that appear after age 35.
Why do I need estrogen? Estrogen is one of the most important hormones for a woman. It protects her against heart attack, stroke, osteoporosis, and Alzheimer’s. It also keeps us looking young and healthy.
Why do I need testosterone? Testosterone is the third female hormone and is as essential as estrogen and progesterone. We need this hormone to keep our thought process quick and our libido healthy. It improves bone density, muscle mass, strength and prevents some types of depression. It is also the source of energy and solid sleep!
Will I grow unwanted hair from testosterone? There is less chance of excess hair growth with natural testosterone than with synthetic hormones. Facial hair will grow with testosterone pellets, but normally no more than when you were in your thirties.
Thank you for trusting us with your hormone therapy. Call us today to schedule your consultation so that you can optimize how you look, feel, and perform as well as reduce your risk of breast cancer, osteoporosis, cardiovascular disease, prostate cancer, and a whole host of other problems!
We have noticed that we end up providing the same education on certain topics over and over. We also noticed that people need to know what we do and how we do it. Against The Grain Podcast is a great solution for this…
People need to know about prolotherapy and bioidentical hormone replacement therapy. They need to know about lifestyle changes. They need to know the different options for thyroid management.
One of our biggest problems is providing this education. I’ve thought long and hard about how to tackle this problem. The solution…
Our podcast if totally free. It is available on iTunes as well as the againstthegrainpodcast.com website. You can download the podcast from the website. You can subscribe to it and listen to it on your phone and in your car. We are trying to provide great content to help with common medical problems.
As of the time of this writing the first few podcast topics are:
Podcast #1: Introduction
Podcast #2: Labs – what is ‘normal’? Have you ever wondered where those normal values came from anyway?
Podcast #3: Prolotherapy – excellent therapy for musculoskeletal pain and injury
Podcast #4: Testosterone Replacement Therapy
Podcast #5: Tamiflu – why it isn’t worth the money and won’t help you get better any faster
Podcast #6: Flu-Shot – why it probably isn’t helpful and reviews the literature showing a strong lack of data
Podcast #7: The Emergency Room – when should you go to the ER and when it may not be the best thing
Podcast #8: Insurance – A Betting Man’s Game. Why insurance isn’t as helpful as you may think but also why you have to have it.
Podcast #9: Thyroid & Synthroid – all you wanted to know about thyroid and hormones
Podcast #10: MRI – not as helpful as you think. MRI can be very helpful but it may not be as helpful as you think
Podcast #11: Low Back Pain – what causes it and what you can do about it
Podcast #12: Diabetes
Podcast #13: Acne & Hormones – why do people get acne when they start hormone replacement?
Podcast #14: Antibiotics for Upper Respiratory Infections (URI) – do you really need those antibiotics or are they more harmful?
Podcast #15: Get Your O Back – far too many women are faking orgasm. This can often be fixed.
Podcast #16: Bad Birth Control – oral contraceptives can cause a whole host of problems
Podcast #17: Knee Pain – prolotherapy helps with most causes of knee pain
Podcast #18: Adrenal Fatigue – this is a very common issue
More are coming! Please go on to iTunes and share our podcast and give us a great rating!
Once patients come in to our Tulsa clinic for prolotherapy they often ask “why don’t more doctors know about this?”
There are several reasons but one of the primary is that there is a thought that there is no evidence that prolotherapy works. You have to understand that physicians are very busy and often don’t have or take the time to read the studies supporting or refuting the scientific evidence. Thus, we often rely on things like the Cochrane Database. the Cochrane Database reviews available literature and draws conclusions about a given topic.
In the case of prolotherapy the Cochrane Database states “When used alone, prolotherapy is not an effective treatment for chronic low-back pain.”(1) That makes it sound like prolotherapy isn’t effective.
However, I have seen the effectiveness of prolotherapy for years and I know just how well it works. The success rate of prolotherapy is in excess of 85%.
So we have a problem. The scientific review states that prolotherapy isn’t effective yet we know it is effective. So what is the real truth?
The answer lies in the studies that have been performed and those that were included in the Cochrane Database. Once you understand these studies it is clear how they came to the erroneous conclusion that prolotherapy doesn’t work.
The largest study on prolotherapy for the low back 110 patients were randomized to receive either saline injections (control group) or dextrose prolotherapy (test group).(3) At the end of the study they found that there was no significant difference between the control group and the test group so the Cochrane Database review inferred that prolotherapy didn’t work. That is typically the point of a randomized trial, to compare an intervention to placebo and see if it works.
The conclusion that prolotherapy doesn’t work based on this study brings up several issues.
First, you have to compare an intervention against a known placebo. Using saline injections cannot be a placebo because we know that there are potential effects. For example, we know that simply inserting a needle into the tissues has a therapeutic effect.(4) However, if you actually read the study you’ll discover that patients in both groups had pain for 14 years on average. You’ll also discover that both groups of patients were very happy with their results.
The authors of the study stated the correct conclusion about the results in the study: “In chronic nonspecific low-back pain, significant and sustained reductions in pain and disability occur with ligament injections, irrespective of the solution injected or the concurrent use of exercises.“(3) In other words prolotherapy works but so do saline injections in this study.
If prolotherapy works and saline injections also work then why not just use saline? Because there are other studies showing significant differences between saline and dextrose prolotherapy injections.(5) Scarpone demonstrated the effectiveness of prolotherapy and these results were sustained for at least 52 weeks.
Another important component of the Yelland study mentioned above (3) is that they limited the amount of solution injected to 10 mL and the average patient only received 7.5 mL. One of the important features of Hackett-Hemwall prolotherapy is its comprehensive approach. It is not uncommon that we will use in excess of 100 mL of solution for a low back prolotherapy procedure. How can we compare a procedure that is only using 10% of what we are using? It is ultimately a very different approach. You simply cannot say one works and one doesn’t when there is such a huge difference in the way these procedures are performed. Tulsa Prolotherapy Testimonials speak for themselves.
George Hackett, MD published a monograph in the 1956 stating a 90% success rate in over 4000 patients without a single complication. These results are consistent with what we see in our clinic.
Physicians today are very “evidence based.” We look for the scientific evidence to support a given therapy. The problem is that many of my colleagues often “throw the baby out with the bathwater.” In other words, a common thought is that if there is no evidence to support the therapy they won’t do it at all. I can’t tell you how many times I’ve heard “well there’s no evidence it works.”
A lack of evidence is NOT evidence against. In other words, just because there isn’t enough evidence to PROVE something works does not mean that it doesn’t work.
Studies on prolotherapy are difficult for several reasons. It is nearly impossible to ‘double blind’ where neither the prolotherapist nor the patient know if they are getting prolotherapy yet make sure that there is absolutely no benefit with the ‘control’ injection. That point is discussed above.
Second, large scale studies of this kind are very difficult and expensive. The bottom line is that there is no money to be made by performing this study so nobody is going to pay for it. That means we don’t have many studies that prove prolotherapy works. But again, a lack of evidence isn’t evidence against.
In fact, there is danger in not using certain therapies simply because there aren’t sufficient studies proving their effectiveness. This point is well made by a study published in the British Medical Journal (BMJ). The authors reviewed studies on the use of parachutes to prevent death in sky-diving and airborne activities. They found no studies proving the effectiveness and stated:
“As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomized controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organized and participated in a double blind, randomized, placebo controlled, crossover trial of the parachute.“(6)
I think it is funny that the authors basically told those who ignore observational data in absence of randomized controlled trials to go jump out of an airplane without a parachute.
We have to do better than this. We simply cannot throw the baby out with the bathwater!
When it comes to chronic pain you have a few options. You can try physical therapy, medications, natural therapy, accupuncture, massage, chiropractic, surgery, and prolotherapy. There may be others not mentioned as well. Our recommendation is that patients seek the highest success procedure with the lowest cost and the least risk. We believe prolotherapy meets all of these criteria and is worthy of primary consideration.
Prolotherapy is very low-risk, extremely cost-effective, and it works. You have nothing to lose and everything to gain!
Tulsa Prolotherapy is an excellent procedure to help reduce pain and improve function. Prolotherapy has helped countless patients eliminate their pain and it may be the ideal solution for you. Prolotherapy is a minimally invasive, in-office procedure which stimulates your body’s natural healing mechanisms.
Prolotherapy is a simple, safe, and straight forward procedure when administered by a trained prolotherapy practitioner. There are risks associated with virtually any medical procedure. Physicians who are well trained typically have the lowest risk of complication.
Did you know…
Any physician (and many other allied health providers) can say they perform prolotherapy? Also, there is no actual prolotherapy certification. Clearly you want the most qualified person performing your prolotherapy. While prolotherapy is very low risk in the hands of a well trained prolotherapist there is significant risk if not performed correctly.
In the words of C. Everett Koop, MD (former Surgeon General of the US) “The nice thing about prolotherapy, if properly done, is that it cannot do any harm.” The key words here are “properly done.” That is the key.
Dr. Edwards has been performing prolotherapy for several years and has performed thousands of procedures without a single serious complication. Because of that experience he understands how things could go wrong if done incorrectly. That is why he sought out the best training available through the Hackett Hemwall Foundation. He is the ONLY prolotherapist recommended by the Hackett Hemwall Foundation in Oklahoma, much less the Tulsa area.
When you are looking for someone to perform your prolotherapy here are some factors to consider:
What is their training in prolotherapy?
Do they do continuing education in prolotherapy?
How many procedures do they perform on a weekly basis? High treatment volume is generally a good thing.
Are there areas in the body that they do not treat? You want someone who is comprehensive in their approach.
What is their experience with complicated injections?
Do they know how to treat complications they may cause?
Dr Edwards has years of experience in the ICU, hospital wards, Emergency Room, and outpatient clinics. He has seen multiple complications from procedures and knows how to treat them. While you don’t want to be one of the ones with a complication it is important that your prolotherapy provider knows how to treat any possible complication in the low chance one occurs. Simply knowing this helps lower the likelihood that a complication will arise from the procedure because we know what to avoid.
We have seen numerous patients who were treated by other prolotherapy providers and did not improve. However, most of the time Dr Edwards has improved their symptoms if not resolved them all together. We’ve also seen other providers who do not have extensive experience in treating procedural and traumatic complications.
The bottom line
You want the most experienced prolotherapist you can find with the greatest breadth of experience with the prolotherapy procedure as well as identifying and managing potential complications. While these complications are extremely rare in the hands of an experienced prolotherapist the are much higher for inadequately trained providers.
Chronic pain? Sports injuries? Knee, shoulder, neck, or back issues?
These are common reasons people come to us looking for a solution. Tulsa prolotherapy is the solution!
What is Tulsa Prolotherapy?
Prolotherapy is a simply, minimally-invasive, in-office procedure that stimulates your body to heal itself. Prolotherapy has been in Tulsa for more than 10 years. Dr John Merriman was a cardiologist in Tulsa who suffered from neck pain which resolved with prolotherapy. He became an advocate for the procedure and treated hundreds of patients in Tulsa with prolotherapy.
We have found that many patients with pain and injury actually have damaged ligaments and tendons. Due to the relatively poor blood supply these tissues are notorious for not healing completely in many cases. Prolotherapy stimulates the body’s natural inflammatory healing mechanism which repairs these damaged ligaments and tendons.
It doesn’t matter how long ago the injury occurred and it doesn’t matter how long you’ve had pain. Tulsa prolotherapy re-stimulates the inflammatory process healing these damaged tissues. Once the tissues are healed the pain resolves.
How long does Tulsa Prolotherapy last?
If your pain is truly due to damaged ligaments and tendons then when the tissue damage is resolved the pain goes away. The idea is that we restore these tissues to normal. Just like the rest of your body that doesn’t hurt. The results last until you re-injure the area. Dr Hackett, the founder of modern day prolotherapy, performed studies from the 1930’s through the 1950’s. He noted an 85% success rate and these results persisted for over 14 years!
If we are truly healing these damaged tissues then the results last as long as you do.
Why not just have surgery?
Surgery is an excellent option when you know the exact reason you have symptoms. However, this often is not the case. I have seen countless patients with knee pain, neck pain, low back pain, shoulder pain, etc who have had MRIs showing some type of abnormality. The problem is that the abnormalities just don’t always correlate well with the patient’s symptoms.
That is one of the beautiful things about prolotherapy! We can usually identify the exact source of pain because of the way we perform the procedure.
Surgery has risks. I remember a patient who came to see me and she was in a wheelchair and had an above-the-knee amputation of the left leg. I asked her why and she said she had a total knee replacement that got infected and they had to amputate. Ouch!
The first dictum of medicine is “first, do no harm.” In other words do the best you can for the patient but above all don’t do anything to hurt them. We should always look for the fix that has the lowest risk of complications, the least invasive, and the lowest cost.
Prolotherapy is less expensive, has lower risk, is less invasive, and often has a much higher success rate.
Personally, I wouldn’t have surgery until I have maximized the benefit of prolotherapy. You may still need surgery if you aren’t getting benefit with Tulsa prolotherapy. But that is rare!
Can’t I just take naprosyn (or any other NSAID) for my pain?
Not if you want to get better! All anti-inflammatory medications inhibit the inflammatory process. In fact, anti-inflammatory medications (NSAIDs) can block the healing process. Inflammation is part of the healing process and you don’t want to slow or block your healing in any way. We recommend avoiding anti-inflammatory medications for any musculoskeletal issue.
If you have any pain or injury then you should strongly consider prolotherapy in our Tulsa, Oklahoma clinic. Our patients typically have excellent results (read their testimonials here).
Jeff is a patient at our Tulsa clinic where we perform prolotherapy frequently. He had a long history of low back pain. He also had pain radiating down his leg which was described as sciatica. He was concerned that he may have a herniated disk in his low back but didn’t want surgery to repair it.
After a thorough evaluation it was determined that Tulsa Prolotherapy could help him.
3 rounds later his pain was nearly completely gone!
Many patients wonder if their particular issue could eventually go away. There are no guarantees but prolotherapy is your best chance.
If you have back pain, sciatica, or any other pain for that matter then you should really consider prolotherapy. It is very safe and effective!
It is old news that since the passing of the Affordable Care Act in 2010, health insurance premiums and deductibles are on the rise. But what you may not know is you can save money by paying cash for your healthcare regardless of whether or not you have health insurance. Here’s 4 ways to save at Revolution. 1. Lower office visit rates.
We bill for time which is considerably more affordable than many patient’s experience in an “In-Network” office setting regardless of their health insurance status. Traditional medical billing is based on the number of criteria met during the documentation of the visit. If your doctor clicks enough boxes in their electronic medical record (EMR) then they can bill more for it. However, clicking boxes doesn’t mean they have more thoroughly addressed your issue!
We focus on YOU and our time with you not the number of boxes we check in your record.
2. Free lab work.
It’s not uncommon for those going to traditional insurance-based offices for healthcare to be billed hundreds of dollars for even basic lab work. As long as patients have some type of insurance, even high deductible health plans, Revolution provides advanced comprehensive lab testing at no cost to the patient in many cases. If a patient does not have insurance, we have contracted lower lab testing rates that can save hundreds in testing fees.
Feel free to shop around but you will be hard pressed to find a better deal on labs anywhere!
3. True Wellness.
It’s no secret that prevention is the best medicine. At Revolution, our comprehensive lab testing programs allow for each patient to understand current status of their overall health and specific ways to not only prevent disease but reverse disease.
For instance, over 11% of Oklahomans have diabetes and even more have pre-diabetes. In a study published in the Diabetes Journal it’s estimated that an individual’s lifetime medical expenses for this one disease process is anywhere from $43,000 to over $211,000 depending on the age of onset of disease process.
Additionally, many who have diabetes will also have other co-morbid conditions such as heart disease. Not only, can Revolution help you prevent the disease but often greatly improve the disease, if not reverse the process thus saving big money!
4. Membership
We now have membership plans available to provide patients health services for a discounted yearly fee or monthly payment. This allows you to know up front how much your optimal health will cost you and allow you to incorporate this into your budget. Knowing how much it costs can dramatically reduce a lot of stress.
Stay tuned for more information or call 918.935.3636 to learn more!
There is a lot of negative information floating around out there about testosterone supplementation and possible negative effects of testosterone replacement with recent attention on cardiovascular disease and heart attacks.
I hope to clear up some of this information in this post.
A recent study publish by Finkle showed an increased risk of heart attacks in older men after starting testosterone. I’ve previously discussed several problems with this study in Does Testosterone Cause Heart Attacks.
The FDA has noticed the information about testosterone and cardiovascular disease and issued a warning about the possible cardiovascular effects of testosterone replacement therapy in March, 2015.(1) However, the European stance on testosterone is quite different. The Coordination Group for Mutual Recognition and Decentralized Procedures–Human (CMDh) stated that there is “no consistent evidence” of an increase in heart related problems associated with testosterone replacement.(2)
In one of the most profound statements I’ve seen in a while, the FDA stated “Patients using testosterone should seek medical attention immediately if symptoms of a heart attack or stroke are present, such as chest pain, shortness of breath or trouble breathing, weakness in one part or one side of the body, or slurred speech.”(2)
Seriously?
I’m pretty sure that ANYONE experiencing “symptoms of a heart attack or stroke are present, such as chest pain, shortness of breath or trouble breathing, weakness in one part or one side of the body, or slurred speech” should seek medical attention immediately. Did they really need to make that statement?
All of this represents an issue that I believe is far too common… a rush to judgement on the weakest bits of evidence possible.
I wish they would apply the same level of scrutiny to prolotherapy. Maybe then it would be a covered benefit for most patients.
All of this concern about testosterone replacement causing heart attacks started with an article published in 2013 in JAMA.(4) 8709 men in the VA system with low testosterone and had undergone coronary angiography were followed for 3 years. The researchers noted the absolute rate of stroke, heart attack, and death to be 25.7% in patients who had been prescribed testosterone. However, they reported the rate of 19.9% (5.8% lower) in patients who hadn’t received a testosterone prescription.
Sounds like a big deal…
There was a lot of media attention about this data. The problem is that these numbers are inaccurate.
The correct absolute rate of events (number of events divided by the number of patients) was over 50% less in the testosterone treated group (10.1% vs 21.2%).(5)
JAMA has published 2 follow up articles attempting to discuss and correct errors in the data. Interestingly, the “all-male” population of the study actually contained almost 10% women.(6) At least 29 medical societies have stated that the data has lost credibility and called for a retraction of the article.(7)
In regards to the Finkle study mentioned earlier… Let’s just say that there were so many methodological concerns in how they analyzed the data that the FDA stated “…it is difficult to attribute the increased risk for non-fatal MI seen in the Finkle study to testosterone alone…”(8)
There are lots of studies on testosterone. But there are only 4 which suggest an increased risk of cardiovascular disease associated with testosterone replacement. These results are inconclusive and intermixed with a number of problems.
On the other hand, there are lots of studies that show benefit.
There is an increased risk of mortality, atherosclerosis, and coronary artery disease in patients with low testosterone.
Men treated with testosterone have a 50% reduced mortality when compared with men not treated with testosterone.
In men with known heart disease exercise capacity increased with with testosterone replacement vs placebo
Cardiovascular disease risk factors such as fat mass, waist circumference, and insulin resistance improve uniformly with testosterone replacement vs placebo.(9)
Despite this evidence there is a negative view on the use of testosterone. You may have seen the lawyer advertisements asking men who have suffered a stroke or heart attack and been on testosterone to contact them.
Many patients have stopped taking testosterone and many physicians have stopped prescribing it. Those who continue to prescribe may be viewed negatively by their peers.
In a recent article by Abraham Morgentaler, MD it was reported that testosterone replacement therapy had level 1 evidence supporting its use for improving libido, erection, mood, increased muscle mass, increased bone density, and reduced fat mass.(3)
There are numerous benefits (sexual and non-sexual) to testosterone replacement that are well validated in the literature. Testosterone replacement not only improves symptoms but also improves overall health. There is no clear evidence that testosterone replacement is associated with increased risk of prostate cancer or cardiovascular disease.
Known risks of testosterone replacement include: gynecomastia, erythrocytosis, acne, peripheral edema, reduced fertility, and reduced testicular size.
In most cases, the risks of testosterone replacement therapy are far outweighed by the benefits. However, this is a very individual decision between you and your doctor.
If you think you have symptoms of low testosterone then call us today to schedule your appointment.
Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310;1829-1836.
Traish AM, Guay AT, Morgentaler A. Death by testosterone? We think not! J Sex Med. 2014;11:624-629.
Correction. Incorrect number of excluded patients reported in the text and figure. JAMA. 2014;311:967. http://jama.jamanetwork.com/article.aspx?articleid=1835478 Accessed May 29, 2015.
Morgentaler A, Lunenfeld B. Testosterone and cardiovascular risk: world’s experts take unprecedented action to correct misinformation. Aging Male. 2014;17:63-65.
US Food and Drug Administration. Citizen petition denial response from FDA CDER to public citizen. July 16, 2014. http://www.regulations.gov/#!documentDetail;D=FDA-2014-P-0258-0003 Accessed August 31, 2014.
Morgentaler A, Miner MM, Caliber M, Guay AT, Khera M, Traish AM. Testosterone therapy and cardiovascular risk: advances and controversies. Mayo Clin Proc. 2015;90:224-251.
Tendonitis refers to damage to the tendons in the shoulder. Prolotherapy is particularly beneficial in these cases because it stimulates the healing process of these tendons.
The term ‘tendonitis’ refers to inflammation of a tendon. However, the term is often used inappropriately because there is not always inflammation despite the fact that there is pain. A better term would be tendonosis – meaning an abnormal condition of the tendon.
It could be due to over use. It could be due to a specific injury. Regardless, the shoulder hurts and it is due to something wrong with the tendon. So what do you do about it?
Tendonitis Treatment Options
Typical treatments of shoulder tendonitis include avoiding painful activities, ice or cold packs, anti-inflammatory medications (NSAIDs), physical therapy, and surgery.
If you’ve been reading my posts on prolotherapy for shoulder injuries then you’ll recognize those therapies listed above as the staple therapy for most shoulder injuries. Sometimes these therapies work. However, I’m not a fan of steroid injections for these conditions and I only recommend surgery as a last resort.
I’ve discussed the importance of good ligament and tendon health many times. You may recall that these ligaments and tendons are very densely innervated with nerves. When these ligaments and tendons are damaged they become irritated which irritates the nerves within them which are very susceptible to pressure and stretching.
After an injury we should heal.
We have a healing mechanism. It is called inflammation. The inflammation produces a number of chemicals and responses that initiate the process of healing. However, this healing process is often incomplete depending on the person and the injury.
The healing is incomplete for a number of reasons but one of them is the poor circulation inherent in these ligaments and tendons. Under normal circumstances they do not need a good blood supply. They are not metabolically active even during exercise. They are like steel cables. They don’t require energy, at least not very much.
If they don’t heal well then the injury persists and so does the pain.
Your options are listed above. Or you could consider prolotherapy. In many cases it is your best option for shoulder tendonitis.
Our success rate for shoulder injuries, including shoulder tendonitis, is very high. In excess of 90%. Prolotherapy has an excellent track record for improving pain and function with very little potential for complications if it is done correctly.
The success rate is not 100% (though it is very high) but it is certainly worth a try when you consider the down time, deductibles, physical therapy time, risks, and so on.
What have you got to lose?
Call our office today so that we can evaluate your shoulder for tendonitis and see if prolotherapy is right for you!
We treated a lot of shoulder injuries at our Tulsa clinic. Adhesive capsulitis, also known as ‘Frozen Shoulder’, is a cause of restricted range of shoulder motion and pain.
We aren’t exactly sure what causes a frozen shoulder (adhesive capsulitis) but we do know that it results in scar adhesions in the shoulder joint capsule reducing the ability of the arm to rotate in the shoulder socket.
In my experience, most of these frozen shoulders started with the onset of shoulder pain which made the patient not want to move their shoulder. This, coupled with the inflammation associated with the cause of the pain, results in these adhesions forming around the joint capsule.
A tell-tale sign of a frozen shoulder is that both active and passive range of motion are both equally decreased. This is fairly easily evaluated during the physical exam.
How do you treat adhesive capsulitis (frozen shoulder)?
There are 2 primary targets for treating adhesive capsulitis:
Increase range of motion
Reduce pain
There are a number of therapies commonly used to help with both of these. Physical therapy can be helpful for increasing range of motion. Anti-inflammatory medications (NSAIDs) are often prescribed. Some patients may get steroid injections which may be beneficial in some cases. Massage therapy and daily stretching techniques may help.
I don’t recommend steroid injections for musculoskeletal issues. Steroids are damaging to the tissues and make them weaker. I recommend avoiding steroids at all costs for these kinds of issues.
These adhesions can be broken under sedation in the operating room if they don’t improve. For really bad cases surgery could be considered to break down these adhesions.
I don’t recommend surgery very often. There are just too many risks most of the time. However, surgery certainly has its place and can be fabulous. It just needs to be used appropriately.
Prolotherapy for frozen shoulder?
There is another therapy that has been shown to be very beneficial but not well know. Prolotherapy can be a tremendous benefit for frozen shoulders.
While prolotherapy by itself won’t increase the range of motion it can have a dramatic and profound impact on the pain which can allow increased efforts on stretching and mobilization techniques.
We have treated numerous patients with adhesive capsulitis and prolotherapy has provided them exceptional benefit. Prolotherapy is my first recommendation for nearly all causes of shoulder pain but certainly with frozen shoulders.
There is next to no risk associated with prolotherapy. It is extremely cost effective and often very successful.
If you have a frozen shoulder then you should consider prolotherapy as it can melt away this painful condition.
Call our clinic today to schedule your evaluation.
Shoulder impingement is one of many possible causes of shoulder pain.
Or is it?
Shoulder impingement, so the story goes, is caused by a narrowing of the subacromial space when the arm is abducted or lift your arm away from your body sideways.
This action raises the greater tubercle of the humerus and closes in on the subacromial space which, in theory, compresses the supraspinatus tendon causing pain and irritation.
I argue that the impingement has its roots in damaged ligaments and tendons. There are several of these structures in the area that could make it seem like impingement was the issue. Maybe it is impingement but WHY is it getting impinged. Because of weakened and/or damaged tendons and ligaments.
How do you diagnose shoulder impingement?
Shoulder impingement is typically diagnosed by the history and physical exam. It is a clinical diagnosis. 2 common tests used to evaluate for impingement are Hawkin’s and Neer’s signs. If symptoms are reproduced with these tests then it is suggestive of rotator cuff disease. MRI may or may not be helpful and I rarely order them for this type of shoulder pain.
How do you treat shoulder impingement?
Shoulder impingement is often treated initially with conservative therapy which consists of rest, physical therapy, taping, acupuncture, and avoiding doing anything that causes pain. If that doesn’t work then anti-inflammatory medications (NSAIDs) are often given and the patient may get a steroid shot. Sometimes the steroid shots work but they often don’t.
I vividly remember being taught how to do a steroid injection for shoulder pain when I was in residency. I was taught a single technique in a single location for the shoulder. That may work well when the painful or damaged area is the area I happen to inject the steroids. But it often isn’t.
Why did I learn a single injection and assume that it would fix all potential issues that a shoulder may help with? That makes absolutely no sense. I clearly wasn’t thinking!
If these techniques don’t work then surgery may be recommended.
Prolotherapy for shoulder impingement?
I strongly recommend prolotherapy for potential shoulder impingement issues. In fact, I can’t think of a shoulder that we didn’t help for shoulder impingement. It is just that good.
Prolotherapy stimulates your body to heal itself through its own natural inflammatory process. It can strengthen the weakened and damaged ligaments and tendons that are causing the problem to begin with. When these tissues are healed through the body’s normal healing processes then the pain goes away and full function is restored.
We treat a LOT of shoulders with prolotherapy. We’ve had good enough success with prolotherapy for shoulder pain, SLAP lesions, rotator cuff tears, and shoulder impingement that I just won’t recommend surgery until after the patient has failed prolotherapy. It is rare but it can happen.
Plus, remember that prolotherapy has very little risk. In fact, C. Everett Koop, MD, the former Surgeon General of the United States, stated “the nice thing about prolotherapy, if done correctly, is that it cannot do any harm.”
There is very little risk, basically no downtime, very cost effective. Why don’t you call us to be evaluated for prolotherapy for your pain?
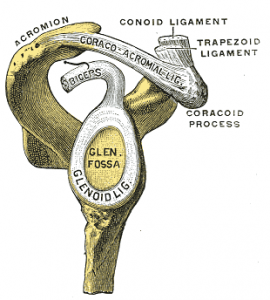
“Gray328”. Licensed under Public Domain via Wikimedia Commons – http://commons.wikimedia.org/wiki/File:Gray328.png#mediaviewer/File:Gray328.png
SLAP lesions or SLAP tears are a someone common cause of shoulder pain. At least that is what the MRI tells us. We see it all the time.
The shoulder is the most frequently injected area (with prolotherapy) in our clinic. One reason is that the shoulder is somewhat commonly injured due to its structure. You can read more about the shoulder anatomy on our Prolotherapy for Rotator Cuff Injury post.
The typical course is that you start to get shoulder pain either from an injury or it just starts hurting for no apparent reason. You go to your doctor and get physical therapy, steroid injections, NSAIDs (anti-inflammatory medications), etc. These things sometimes help and that may be all you need.
But many people aren’t so fortunate. These people are often referred for an MRI and to the orthopedic surgeon. They find a SLAP lesion on your MRI and recommend surgery.
What is a SLAP lesion?
SLAP stands for Superior Labrum tear from Anterior to Posterior. You can see from the image above the ‘Glenoid Lig.’ This is actually the labrum. It is the cartilage in the shoulder which is somewhat analogous with the meniscus in the knee. You’ll also notice something coming off the top of it in that picture.
The structure coming off the top is the long head of the bicep. When the stress on the tendon exceeds its capability then something has to give.
There are several ‘sub-types’ of SLAP lesions depending on the specific location of the injury.
What can you do for a SLAP tear?
You have a few options for what you can do about your SLAP lesion. Traditional approaches involve physical therapy and/or surgery. Wikipedia states “Few with SLAP lesion injuries return to full capability without surgical intervention. In some, physical therapy can strengthen the supporting muscles in the shoulder joint to the point of reestablishing stability. For most others, the choice is to do nothing or some form of surgical repair.”
But when you overlay the information about the success of MRI in identifying these lesions we should certainly consider other options.
Prolotherapy for SLAP tears:
The goals of prolotherapy are to decrease pain and improve functionality. Prolotherapy is VERY good at doing that. There are no studies proving that Prolotherapy ‘cures’ SLAP lesions. In my opinion, there is no reason to do that study.
Why? Well, do you care if your MRI is ‘abnormal’ if you have full function, strength, and range of motion and you don’t have any pain?
Prolotherapy stimulates the body’s natural healing mechanisms and has a very high success rate for dramatically improving the pain and decreased functionality associated with SLAP lesions.
We have treated numerous patients with shoulder pain and MRI diagnosed SLAP tears with excellent results. We have returned numerous athletes to their game in record time without any down time. Several college athletes were able to keep their scholarship because of prolotherapy. They assured me that they were going to lose it if we couldn’t help them.
If you have been diagnosed with a SLAP tear or you have shoulder pain then you should be evaluated for prolotherapy by a qualified and trained prolotherapist.
Check out the Prolotherapy page for more information on how prolotherapy can help your rotator cuff injury and where you can get prolotherapy performed in Tulsa, OK.
Ok, so your shoulder hurts. It is a common issue and we hear the stories every day. There are lots of reasons why your shoulder may hurt and rotator cuff injuries are only one of the many reasons your shoulder may have pain.
At Revolution Health & Wellness Clinic we use a different approach to get our patients back to full function without pain and we usually achieve these goals without surgery!
It is important to understand what is going on with the rotator cuff injury or rotator cuff tear so that prolotherapy makes more sense for this cause of shoulder pain.
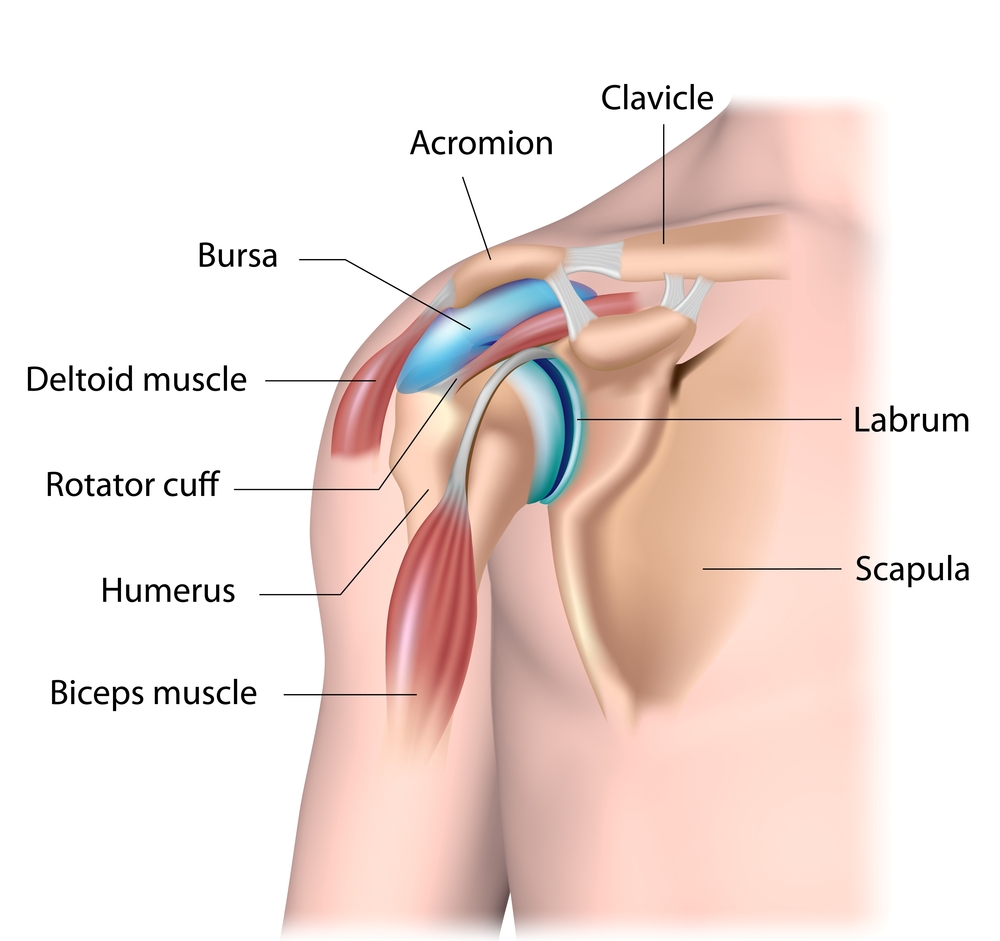
What is the Rotator Cuff?
The shoulder joint is a ball and socket type of joint just like the hip. However, you’ll notice that the shoulder has a lot more range of motion than the hip. The ability for your shoulder to move like it does requires a different anatomy. The socket isn’t much of a socket really. This is one reason you can move your arm like you can.
This range of motion comes at a cost though. We lose some stability in the shoulder joint in order to achieve this increased functionality. Something has to try to hold that shoulder together.
Enter the rotator cuff
The rotator cuff is composed of 4 tendons which help hold the shoulder together. Many medical professionals call these tendons (attached to muscles) the SITS muscles:
Supraspinatus
Infraspinatus
Teres minor
Subscapularis
Each of these tendons provides additional support and structure to the shoulder while allowing this increased motion. However, these tendons are prone to damage and tearing due to the strain often placed on them.
The typical story is that your shoulder starts hurting. Sometimes it is due to a specific injury and sometimes your shoulder just starts hurting. Regardless, you go to your doctor who takes a look at it. You may get a steroid shot. Sometimes that helps and sometimes it doesn’t. If you don’t get better you may be sent to physical therapy or to an orthopedic surgeon. Sometimes you get an MRI. Yet your shoulder still hurts.
What is the deal with the rotator cuff and why does it hurt?
The rotator cuff is made of tendons as explained above. These tendons are very densely innervated with nerves. I talk more about this on the ‘How does prolotherapy work?‘ page.
When these tendons are damaged it irritates the nerves which are very sensitive to pressure and stretching. Sometimes this damage is due to a partial or a full thickness tear. Sometimes it is simply irritation of the tendons themselves.
It could be damage to any of the rotator cuff tendons that is causing the symptoms. Fixing the shoulder pain requires addressing all of the damage. Prolotherapy is very good at doing that. It is a very comprehensive procedure.
Prolotherapy is specifically designed to stimulate the healing process for these rotator cuff tendons. Animal studies have shown that prolotherapy can make the tendon 40% thicker and 50% stronger than it was.
That is great news for a condition that is due to tendon damage.
If you have shoulder pain or a rotator cuff tear or rotator cuff injury then you should strongly consider prolotherapy.
There is minimal risk. It is cost effective (>90% success rate in our clinic), simple, and well tolerated. Plus, there is no down time or recovery after the procedure. You don’t even have to take time off!
So what are you waiting for? Call our clinic so we can get you on the path to healing that damaged rotator cuff.
Here are a couple of people who wanted to share their story with their shoulder pain:
Chromium is an essential trace mineral that plays an important role in optimizing insulin function and the regulation of blood glucose levels. Chromium may also be anti-atherogenic and assist in lowering cholesterol. Following food intake, blood glucose levels rise causing insulin to be secreted by the pancreas. Insulin lowers blood glucose levels by increasing the rate at which glucose enters a person’s cells. Chromium is believed to facilitate the attachment of insulin to the cell’s insulin receptors. Studies also indicate that chromium participates in cholesterol metabolism, suggesting a role for this mineral in maintaining normal blood cholesterol levels and preventing atherosclerosis. Chromium also plays a role in nucleic acid synthesis.
Deficiency Symptoms:
Due to processing methods that remove most of the naturally occurring chromium from commonly consumed foods, dietary deficiency of chromium is believed to be widespread in the United States. Chromium deficiency may increase the likelihood of insulin resistance, a condition which the cells of the body do not respond to the presence of insulin. Insulin resistance an lead to elevated blood levels of insulin (hyperinsulinemia) and elevated blood levels of glucose, which can ultimately cause heart disease and/or diabetes. Deficiency of chromium is associated with metabolic syndrome. Metabolic syndrome represents a constellation of symptoms, including hyperinsulinemia, high blood pressure, high triglyceride levels, high blood sugar levels, and low HDL cholesterol levels. These symptoms increase one’s risk for heart disease. Low levels of chromium are also associated with an increased risk of coronary artery disease incidence and mortality.
Chromium deficiency correlate with depressed nucleic acid synthesis. Chromium is essential for maintaining the structural stability of proteins and nucelic acids and animal studies have found that this element is also vital for healthy fetal growth and development. Studies on humans have established that premature infants and those with evidence of intrauterine growth retardation have significantly lower chromium status compared to infants born full-term. Others have found that multiparous women have far lower body chromium levels compared to nulliparous women. These findings suggest that chromium is an essential trace element during fetal growth and development.
Repletion Information:
In 2001, the Institute of Medicine at the National academy of Sciences conducted a thorough review of the chromium research can concluded that excessive intake of chromium from foods or supplements is not associated with any adverse effects. As a result, to Tolerable Upper Intake Level (UIL) was established for this mineral. However, people with liver or kidney disease may be more susceptible to adverse effects from excessive intake of chromium, and such individuals are cautioned to avoid taking more than 200 micrograms of chromium supplements per day. There is limited evidence to suggest that long-term chromium picolinate supplementation at levels greater than 200 micrograms per day may also be hazardous to chromosome integrity and should be avoided.
We deal with Glutathione in our clinic in Tulsa Functional Medicine Clinic frequently. Why? What is glutathione and what does it do?
Reduced glutathione, commonly known as glutathione or GSH, is a tripeptide (3 amino acids) consisting of L-glutamine, L-cysteine, and glycine. It is ubiquitous in living systems.
Glutathione biosynthesis can be affected by biochemical individuality and/or dietary factors. Chronic oxidative stress can also deplete cellular glutathione. Precursors to glutathione, such as whey protein, vitamin C, and glutamine, are often recommended to boost glutathione levels in the body; however, results are inconsistent.
Biological individuality is such that not every body has equivalent ability to metabolize the precursors to raise glutathione.*
Glutathione has numerous cellular function benefits including antioxidant protection and detoxification. It is essential for the maintenance of cell membrane integrity in red blood cells.
Intracellular glutathione concentrations (as determined by the Spectracell test) are principally derived by intracellular synthesis, as few cells directly uptake glutathione from the surrounding extracellular fluid. The high concentration of glutathione in virtually all cells clearly indicates its importance in metabolic and oxidative detoxification processes.
Glutathione is considered the “Master Antioxidant.”
Deficiency Symptoms
A wide range of human conditions such as aging, cancer, atherosclerosis, arthritis, viral infections, AIDS, cardiovascular, neurodegenerative diseases and pulmonary diseases may be produced, or made worse, by “free radicals.”
The treatment or prevention of these conditions often includes antiooxidants such as Vitamin C, Vitamin E, carotenoids, and selenium. Glutathione is an essential component of the antioxidant defense system producing a “sparing effect” for both tocopherol and ascorbate by reducing the oxidized forms, and by eliminating hydrogen peroxide by reacting with glutathione peroxidase.
Cellular glutathione functions to decrease the formation of oxidized LDL, implicated in the development of atherosclerosis. T-lymphocytes become deficient in glutathione in the prostaglandins from n-3 and n-6 polyunsaturated fatty acids which are important in the inflammatory response.
Patients with adult respiratory distress syndrome are favorably affected by treatments that increase cellular glutathione.
Why Not Give Pure Glutathione?
Glutathione is poorly absorbed from the GI tract and foods rich in glutathione do not appear to contribute to increases in intracellular glutathione levels.
Unfortunately, most oral forms of glutathione are foul smelling, but more importantly, the majority of an oral dose is oxidized before it can be absorbed and used by the cells. This formulation delivers a unique preparation of glutathione that overcomes these usual limitations. The stability of S-acetyl glutathione through the intestinal wall and the plasma is well documented in the literature. Oral intake of S-acetyl glutathione increases total glutathione and percent-reduced glutathione. Percent-reduced glutathione is a very significant biomarker of health status.*[1-5]
Cysteine appears to be the limiting amino acid in the intracellular synthesis of glutathione and supplementation with up to 2000mg daily of N-Acetyl Cysteine appears safe.
Supplementation with normal cysteine is not recommended as it may be poorly tolerated by many patients. In addition, it may be rapidly oxidized to L-cystine, a less usable form for the synthesis of glutathione. Foods rich in cysteine are generally high protein foods such as meats, yogurt, wheat germ, and eggs.
Mechanism of Absorption
S-acetyl glutathione, a lipid-like compound, is taken up intact by chylomicrons in the gut. The acetyl bond is placed on its thiol group or sulfur group, which prevents oxidation and allows the molecule to pass diffusively into the cell after absorption in the gut.
The acetyl bond is then cleaved by non-specific enzymes inside the cell. Acetylation prevents the breakdown of glutathione, and S-acetyl glutathione does not require energy expenditure to be cleaved to reduced glutathione once it crosses the cell wall.*1-8
Antioxidant Activity
Glutathione functions extensively in tissues and organs throughout the body. It plays critical roles in protecting the body from oxidative stress, maintaining cellular functions, and supporting healthy immune function.1,4
Many factors can increase cellular exposure to oxidative insult, and therefore increase cellular consumption of nutrients—such as glutathione—that provide antioxidant activity. This may result in a fierce cycle of oxidative stress and challenges to detoxification. Complete biotransformation and protection from oxidative stress are important to maintaining cellular integrity and tissue health.*2,5
Other Benefits of Maintaining Healthy Glutathione Levels
Much information related to mitochondrial health has surfaced in the literature. Mitochondria, the energy-producing powerhouses of cells, are also the primary intracellular site of oxygen consumption and the major source of reactive oxygen species (ROS). S-acetyl glutathione has been shown to cross the membrane of the mitochondria, increasing the organelle’s activity and minimizing ROS.8,9 Reduction of ROS is associated with maintaining mitochondrial integrity and function, and improved mitochondrial health is believed to support overall health and energy.*
S-acetyl glutathione has also been shown to decrease TNF-alpha, NF-kappa beta, and F-2 isoprostane.4,9-12 Additionally, there is mounting evidence that intracellular glutathione levels in antigen-presenting cells (e.g. macrophages) may influence the Th1/Th2 cytokine response pattern and promote a balanced immune reaction.*10
Directions
Take 2 capsules daily for general support and therapy. For Alzheimer’s prophylaxis, take 1 capsule daily.
References
Locigno R, Pincemail J, Henno A, et al. S-Acetyl-glutathione selectively induces apoptosis in human lymphoma cells through a GSH- independent mechanism. Int J Oncol. 2002 Jan;20(1):69-75. [PMID: 11743644]
Lomaestro BM, Malone M. Glutathione in health and disease: pharmacotherapeutic issues. Ann Pharmacother. 1995 Dec;29(12):1263-73. [PMID: 8672832]
Cacciatore I, Cornacchia C, Pinnen F, et al. Prodrug approach for increasing cellular glutathione levels. Molecules. 2010 Mar 3;15(3):1242- 64. [PMID: 20335977]
Vogel J, Cinatl J, Dauletbaev N, et al. Effects of S-acetylglutathione in cell and animal model of herpes simplex virus type 1 infection. Med Microbiol Immunol. 2005 Jan;194(1-2):55-59. [PMID: 14624358]
Ballatori N, Krance SM, Notenboom S, et al. Glutathione dysregulation and the etiology and progression of human diseases. Biol Chem. 2009 Mar;390(3):191-214. [PMID: 19166318]
Richman PG, Meister A. Regulation of gamma-glutamyl-cysteine synthetase by nonallosteric feedback inhibition by glutathione. J Biol Chem. 1975 Feb 25;250(4):1422-26. [PMID: 1112810]
Anderson ME, Powrie F, Puri RN, et al. Glutathione monoethyl ester: preparation, uptake by tissues, and conversion to glutathione. Arch Biochem Biophys. 1985 Jun;239(2):538-48. [PMID: 4004275]
Anderson ME, Nilsson M, Sims NR. Glutathione monoethyl ester prevents mitochondrial glutathione depletion during focal cerebral ischemia. Neurochem Int. 2004 Feb;44(3):153-59. [PMID: 14568558]
Kretzschmar M. Regulation of hepatic glutathione metabolism and its role in hepatotoxicity. Exp Toxicol Pathol. 1996 Jul;48(5):439-46. [PMID: 8765689]
Fraternale A, Paoletti MF, Casabianca A, et al. Antiviral and immunomodulatory properties of new pro-glutathione (GSH) molecules. Curr Med Chem. 2006;13(15):1749-55. [PMID: 16787218]
Kretzschmar M, Klinger W. The hepatic glutathione system—influences of xenobiotics. Exp Pathol. 1990;38(3):145-64. [PMID: 2192911]
Donnerstag B, Ohlenschlager G, Cinatl J, et al. Reduced glutathione and S-acetylglutathione as selective apoptosis-inducing agents in cancer therapy. Cancer Lett. 1996 Dec;110(1-2):63-70. [PMID: 9018082]
The health of our skin is one of the primary determining factors for looking older. We’ve all seen that person who’s skin makes them look much older than they really are. What causes that?
It is important to understand that your skin ages the most during periods of highest metabolism. Ironically, the time when your skin has the highest metabolism, and therefore the most aging, is during our youth. However, it is never too late! There are benefits to treating your skin regardless of your age.
There are a number of causes for skin aging. But here are the 4 with the most scientific evidence
1) Oxidative Stress
Oxidative stress is an important component of aging all over our body. Inside and out. When it comes to the skin, most of the oxidative damage comes from sun exposure which creates free radicals. In fact, the sun accounts for 85% of these free radicals in the skin.
But don’t forget about toxins. They account for the other 15% of damaging free radicals in your skin. Ultraviolet light (UV) comes in 2 forms and UVA penetrates deeper and causes more oxidative damage.
We can counteract these free radicals with antioxidants. Did know that there are actually a couple of different types of topical antioxidants: hydrophilic and lipophilic. We need both!
Hydrophilic antioxidants (Vitamin C is an example) targets the fluid and spaces in between cells
Lipophilic antioxidants (Vitamin A for example) targets the cell membranes
Taking oral antioxidants is good for your overall health but topical antioxidants are needed in order to address the skin health. You NEED a topical antioxidant for your skin!
When we decrease oxidative damage we see an increase in the health and appearance of the skin. Counteract those free radicals and oxidative damage with:
Pro-Heal Serum Advance+
Super Serum Advance+
2) Inflammation
We simply can’t talk about aging or free radical damage without talking about inflammation. Inflammation is caused by a number of mechanisms and improving those mechanisms can improve the inflammation as well. Free radicals can certainly cause inflammation. Excess inflammation can lead to scarring.
Options for decreasing skin inflammation are:
Pro-Heal Serum Advance+
Extreme Protect SPF 30
Hydra-Cool Serum
3) Glycation
Glycation is simply the process of these glucose molecules attaching to proteins. Proteins throughout the body are glycated based on the level of glucose in the blood or tissues.
Glycation is responsible for a lot of damage incurred in diabetic patients such as cardiovascular disease, retinopathy, neuropathy (nerve damage), and nephropathy (kidney damage). But this same process also damages the skin.
This is a major problem for diabetics but it can be a problem for non-diabetics as well. Collagen is the protein in the skin and it gets glycated as well. Glycated collagen increases wrinkles.
Addressing glycation involves a comprehensive and integrated approach. Skin care products for specifically addressing the glycation of collagen in the skin are:
Youth Complex
Super Serum Advance+
Youth Serum
4) DNA Damage
Many people think of the damage to our skin from sun exposure as the effect on our DNA. One of the problems with UV exposure is the formation of dimers in the genetic material called TT dimers (Thymine-Thymine dimers). There are a number of mechanisms for DNA damage and we need to try to protect our skin from all of them.
Obviously, reducing sun exposure can help with this process. At the same time, sun exposure can be beneficial to our overall health so we have to take that into consideration as well. It is about balance. If you can’t avoid the sun then consider:
Extreme Protect SPF 30
Protective Moisturizer SPF 15
So what do we do about it?
A comprehensive skin care plan should adequately address each of the 4 most common causes of skin aging. Additionally, we should approach our skin health comprehensively and not just from a series of topical solutions we put on our skin.
Revolution Health & Wellness Clinic caries these skin care products and we can definitely help your skin. We carry these products because we believe that there are no greater skin care products available and you definitely deserve the best.

 How do you get Coronavirus Treatment in Tulsa, Oklahoma?
How do you get Coronavirus Treatment in Tulsa, Oklahoma?